

Posterior Scleritis in a Patient with Psoriasis Masquerading as Acute Angle Closure Glaucoma
- PMID: 36845449
- PMCID: PMC9944587
- DOI: 10.1159/000526714
Posterior Scleritis in a Patient with Psoriasis Masquerading as Acute Angle Closure Glaucoma
Abstract
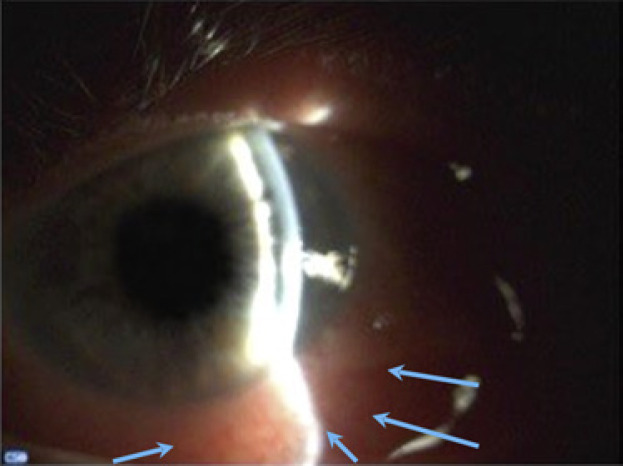
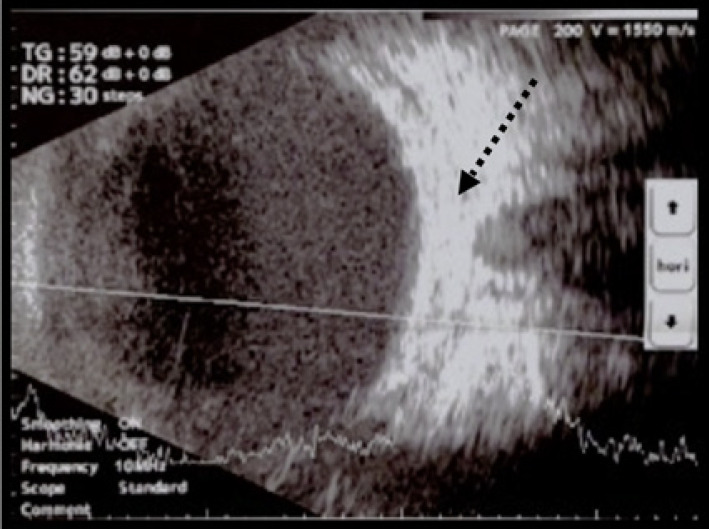
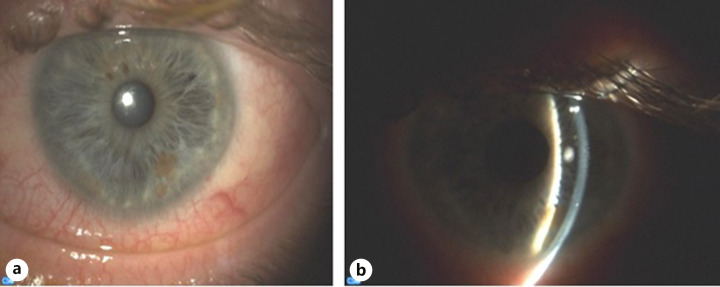
Posterior scleritis is a relatively uncommon form of scleral inflammation of the posterior segment of the eye. Clinical manifestations include ocular pain, headache, pain with ocular movements, and loss of vision. A rare presentation of the disease is acute angle closure crisis (AACC) with elevated intraocular pressure (IOP) secondary to anterior displacement of the ciliary body. Various systemic diseases have been described to co-exist with posterior scleritis; however, psoriasis has not been associated with posterior scleritis. Here, we present a case of posterior scleritis which initially presented as AACC in a patient with pre-existing psoriasis. A 50-year-old male with a history of psoriasis under treatment presented to the emergency department with intense sudden ocular pain and loss of vision on the left eye as well as headache and nausea. A thorough medical and ocular history was taken, and a detailed examination of the anterior and posterior segment was completed including visual acuity and IOP. Initial diagnosis of AACC was made, and appropriate actions were taken with partial resolution of his symptoms. However, upon further work-up including ultrasound (B-scan) of the left eye a final diagnosis of posterior scleritis was made. The patient was treated with steroids and nonsteroidal anti-inflammatory drugs which dramatically improved his condition. Photographic evidence of initial presentation and post-treatment condition was obtained and presented in this report. Posterior scleritis is a potentially vision-threatening condition which is usually challenging to diagnose. In this report, we highlight the challenges one might come into when dealing with different manifestations of the same disease, increasing awareness. This case of posterior scleritis presenting as AACC in a patient with a history of psoriasis enhances what we already know from the literature as well as provides some new insights in the clinical manifestations of posterior scleritis in the setting of psoriasis without arthritis.
Keywords: Angle closure glaucoma; Posterior scleritis; Psoriasis.
Copyright © 2022 by The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Bilateral posterior scleritis presenting as acute primary angle closure: A case report.World J Clin Cases. 2021 May 26;9(15):3779-3786. doi: 10.12998/wjcc.v9.i15.3779. World J Clin Cases. 2021. PMID: 34046483 Free PMC article.
-
Secondary angle closure glaucoma due to posterior scleritis in a case of empty sella syndrome.Nepal J Ophthalmol. 2020 Jul;12(24):308-312. doi: 10.3126/nepjoph.v12i2.26882. Nepal J Ophthalmol. 2020. PMID: 33978626
-
Ciliochoroidal effusion syndrome associated with posterior scleritis.Jpn J Ophthalmol. 2007 Jan-Feb;51(1):49-52. doi: 10.1007/s10384-006-0398-x. Epub 2007 Feb 9. Jpn J Ophthalmol. 2007. PMID: 17295141
-
Nodular Posterior Scleritis Mimicking Choroidal Tumor in a Patient With Systemic Lupus Erythematous: A Case Report and Literature Review.Asia Pac J Ophthalmol (Phila). 2016 Sep-Oct;5(5):324-9. doi: 10.1097/APO.0000000000000165. Asia Pac J Ophthalmol (Phila). 2016. PMID: 26692258 Review.
-
Scedosporium apiospermum infectious scleritis following posterior subtenon triamcinolone acetonide injection: a case report and literature review.BMC Ophthalmol. 2018 Feb 13;18(1):40. doi: 10.1186/s12886-018-0707-4. BMC Ophthalmol. 2018. PMID: 29433463 Free PMC article. Review.
Cited by
-
Posterior Scleritis: A Case Report and Literature Review of the Management of the Condition.Cureus. 2024 Jun 2;16(6):e61537. doi: 10.7759/cureus.61537. eCollection 2024 Jun. Cureus. 2024. PMID: 38831917 Free PMC article.
-
A Rare Case of Posterior Scleritis Masquerading as Acute Angle Closure Glaucoma: Highlighting the Diagnostic Value of Multimodal Imaging.Cureus. 2025 Jun 3;17(6):e85282. doi: 10.7759/cureus.85282. eCollection 2025 Jun. Cureus. 2025. PMID: 40612831 Free PMC article.
References
-
- McCluskey PJ, Watson PG, Lightman S, Haybittle J, Restori M, Branley M. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology. 1999 Dec;106((12)):2380–2386. - PubMed
-
- Gonzalez-Gonzalez LA, Molina-Prat N, Doctor P, Tauber J, Sainz de la Maza M, Foster CS. Clinical features and presentation of posterior scleritis: a report of 31 cases. Ocul Immunol Inflamm. 2014 Jun;22((3)):203–207. - PubMed
-
- Lavric A, Gonzalez-Lopez JJ, Majumder PD, Bansal N, Biswas J, Pavesio C, et al. Posterior scleritis: analysis of epidemiology, clinical factors, and risk of recurrence in a cohort of 114 patients. Ocul Immunol Inflamm. 2016;24((1)):6–15. - PubMed
-
- Boehncke WH, Schon MP. Psoriasis. Lancet. 2015 Sep 5;386((9997)):983–994. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
