

A Rare Geriatric Diagnosis of Eosinophilic Granulomatosis With Polyangiitis: A Case Report
- PMID: 36846640
- PMCID: PMC9957578
- DOI: 10.7759/cureus.35398
A Rare Geriatric Diagnosis of Eosinophilic Granulomatosis With Polyangiitis: A Case Report
Abstract
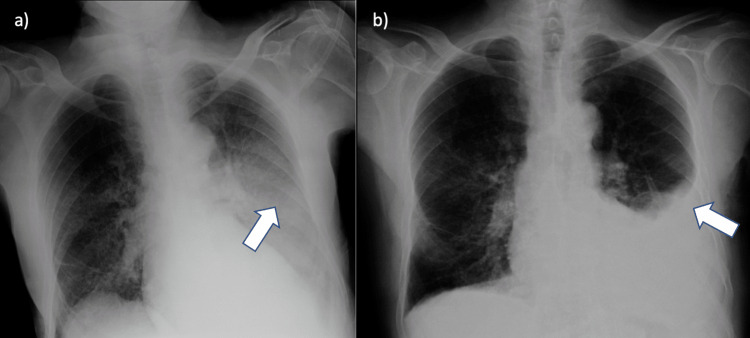
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare form of systemic disease characterized by inflammation and necrotizing effects of the small and medium blood vessels. It is a vasculitis found in all age groups and both genders, although its etiology is unknown. The mean age at diagnosis is 40 years, consisting of an uncommon cause of vasculitis in people older than 65 years. It is the least common of the three antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (EGPA, granulomatosis with polyangiitis (GPA), and microscopic polyangiitis). The characteristic features of EGPA include extravascular eosinophilic granulomas, peripheral eosinophilia, and asthma, usually responsive to steroid treatment. In this article, we discuss a case of an 83-year-old male with a history of undetermined etiology of chronic kidney disease, chronic obstructive pulmonary disease (COPD), and severe chronic rhinosinusitis with nasal polyposis. First hospitalized with the suspicion of community-acquired pneumonia (CAP), based on worsening blood eosinophilia and unresolving respiratory symptoms, a suspicion for EGPA was raised. The development of an eosinophilic pleural effusion, later upon admission, was a predominant factor for its confirmation, as it constitutes a rare finding, only present in about 30% of patients. Laboratory tests showed elevated IgE, the presence of antineutrophil cytoplasmic antibodies directed against myeloperoxidase with a perinuclear staining pattern (ANCA-MPO), and the absence of antiproteinase 3 (anti-PR3) ANCA, which were consistent with the diagnosis. A pleural biopsy was then made, revealing fibrosis with the presence of eosinophils, although with no evidence of granulomas. According to the most recent and accepted classification criteria, the "2022 American College of Rheumatology and European Alliance of Associations for Rheumatology (ACR/EULAR) for EGPA," this patient presented with a score of 13 (a score greater than or equal to 6 is needed for the classification of EGPA). Hence, a diagnosis of EGPA was assumed, and the patient was initiated on corticosteroid therapy, with a favorable response. The aim of this article is to present a rare case of EGPA diagnosis made at the age of 83 years old, although there was evidence that could point to this disease years before the diagnosis was made. In the present case, it is important to point out the long diagnostic delay in a geriatric patient, much older than the median age of diagnosis for EGPA, culminating in a curious case of uncommon pleuroparenchymal involvement.
Keywords: allergic granulomatous angiitis; churg-strauss syndrome; eosinophilic granulomatous vasculitis; geriatric; pulmonary eosinophilia.
Copyright © 2023, Emidio et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Torasemide-induced Vascular Purpura in the Course of Eosinophilic Granulomatosis with Polyangiitis.Acta Dermatovenerol Croat. 2022 Sep;30(2):116-118. Acta Dermatovenerol Croat. 2022. PMID: 36254546
-
Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss Syndrome).2024 Sep 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Sep 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30725784 Free Books & Documents.
-
The Reclassification of Patients With Previously Diagnosed Eosinophilic Granulomatosis With Polyangiitis Based on the 2022 ACR/EULAR Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis.J Rheumatol. 2023 Feb;50(2):213-218. doi: 10.3899/jrheum.220560. Epub 2022 Sep 15. J Rheumatol. 2023. PMID: 36109070
-
A rare case report of polyangiitis overlap syndrome: granulomatosis with polyangiitis and eosinophilic granulomatosis with polyangiitis.BMC Pulm Med. 2018 Nov 29;18(1):181. doi: 10.1186/s12890-018-0733-2. BMC Pulm Med. 2018. PMID: 30497438 Free PMC article. Review.
-
Eosinophilic granulomatosis with polyangiitis.Postgrad Med. 2023 Jan;135(sup1):52-60. doi: 10.1080/00325481.2022.2134624. Epub 2022 Dec 5. Postgrad Med. 2023. PMID: 36259957 Review.
References
-
- Churg-Strauss syndrome. Greco A, Rizzo MI, De Virgilio A, et al. Autoimmun Rev. 2015;14:341–348. - PubMed
-
- Polyarteritis nodosa and Churg-Strauss angiitis: characteristics and outcome in 38 patients over 65 years. Mouthon L, Le Toumelin P, Andre MH, Gayraud M, Casassus P, Guillevin L. Medicine (Baltimore) 2002;81:27–40. - PubMed
-
- The Churg Strauss syndrome (allergic granulomatous angiitis): review and update. Abril A, Calamia KT, Cohen MD. Semin Arthritis Rheum. 2003;33:106–114. - PubMed
-
- Churg-Strauss syndrome. Keogh KA, Specks U. Semin Respir Crit Care Med. 2006;27:148–157. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous