

Does Collaboration between General Practitioners and Pharmacists Improve Risk Factors for Cardiovascular Disease and Diabetes? A Systematic Review and Meta-Analysis
- PMID: 36846722
- PMCID: PMC9951619
- DOI: 10.5334/gh.1184
Does Collaboration between General Practitioners and Pharmacists Improve Risk Factors for Cardiovascular Disease and Diabetes? A Systematic Review and Meta-Analysis
Abstract
Objective: To assess whether inter-professional, bidirectional collaboration between general practitioners (GPs) and pharmacists has an impact on improving cardiovascular risk outcomes among patients in the primary care setting. It also aimed to understand the different types of collaborative care models used.
Study design: Systematic review and Hartung-Knapp-Sidik-Jonkman random effects meta-analyses of randomised control trials (RCTs) in inter-professional bidirectional collaboration between GP and pharmacists assessing a change of patient cardiovascular risk in the primary care setting.
Data sources: MEDLINE, EMBASE, Cochrane, CINAHL and International Pharmaceutical Abstracts, scanned reference lists of relevant studies, hand searched key journals and key papers until August 2021.
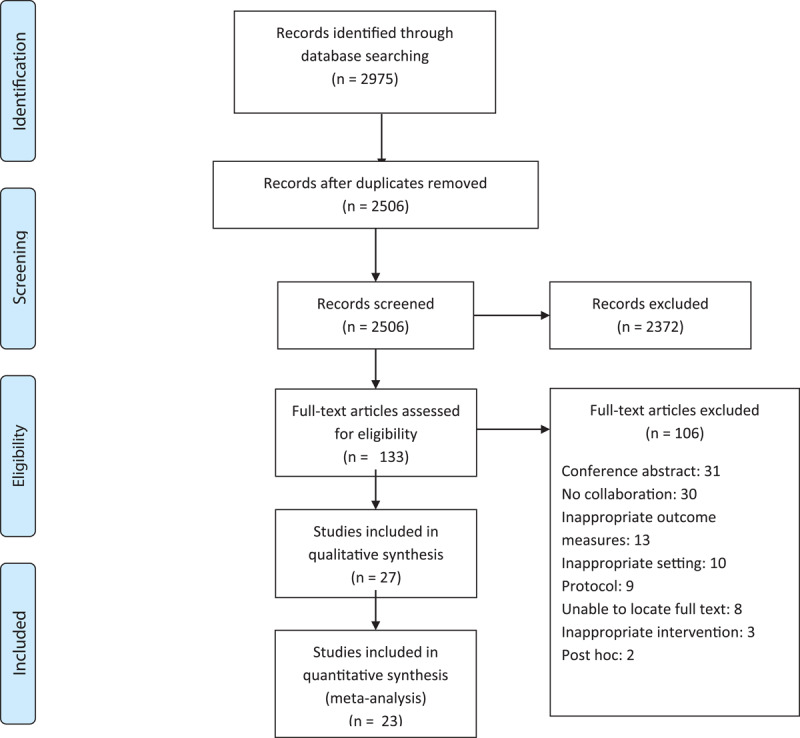
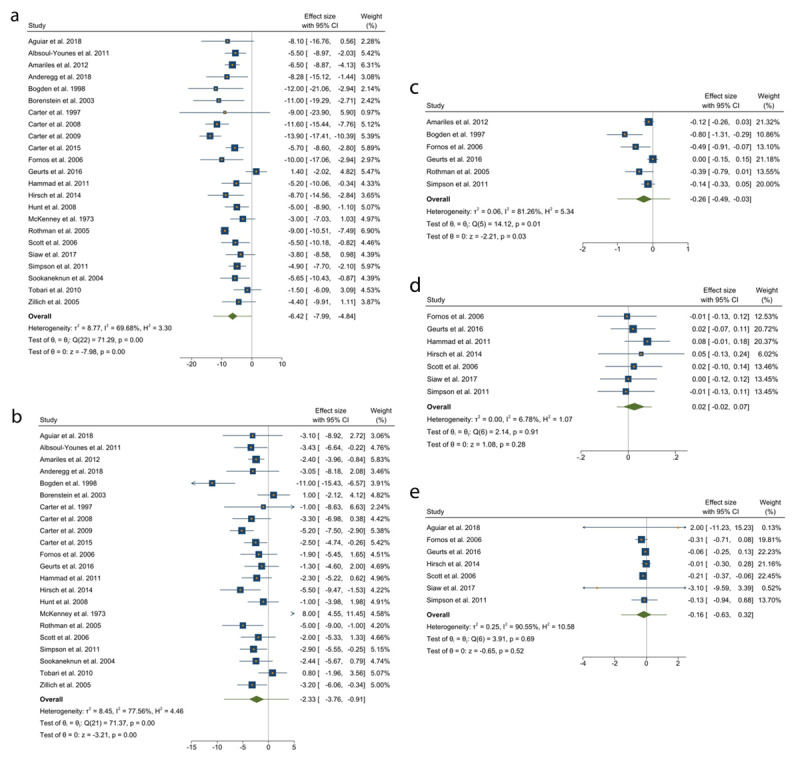
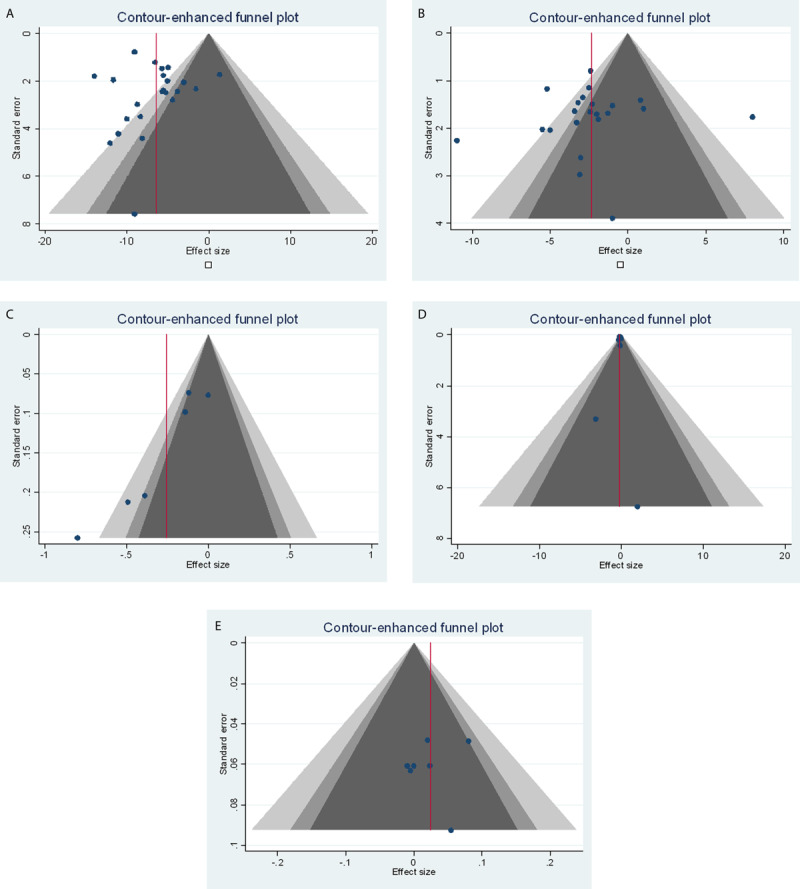
Data synthesis: Twenty-eight RCTs were identified. Collaboration was associated with significant reductions in systolic and diastolic blood pressure (23 studies, 5,620 participants) of -6.42 mmHg (95% confidence interval (95%CI) -7.99 to -4.84) and -2.33 mmHg (95%CI -3.76 to -0.91), respectively. Changes in other cardiovascular risk factors included total cholesterol (6 studies, 1,917 participants) -0.26 mmol/L (95%CI -0.49 to -0.03); low-density lipoprotein (8 studies, 1,817 participants) -0.16 mmol/L (95%CI -0.63 to 0.32); high-density lipoprotein (7 studies, 1,525 participants) 0.02 mmol/L (95%CI -0.02 to 0.07). Reduction in haemoglobin A1c (HbA1C) (10 studies, 2,025 participants), body mass index (8 studies, 1,708 participants) and smoking cessation (1 study, 132 participants) was observed with GP-pharmacist collaboration. Meta-analysis was not conducted for these changes. Various models of collaborative care included verbal communication (via phone calls or face to face), and written communication (emails, letters). We found that co-location was associated with positive changes in cardiovascular risk factors.
Conclusion: Although it is clear that collaborative care is ideal compared to usual care, greater details in the description of the collaborative model of care in studies is required for a core comprehensive evaluation of the different models of collaboration.
Keywords: allied health; cardiovascular disease; collaboration; general practitioner; pharmacist; primary care.
Copyright: © 2023 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
-
- Australian Institute of Health and Welfare. Cardiovascular disease: Australian facts. Cardiovascular disease series Cat no CVD 53. Canberra: AIHW; 2011.
-
- World Health Organization. Prevention of cardiovascular disease: guidelines for assessment and management of total cardiovascular risk; 2007.
-
- Country statistics and global health estimates by WHO and UN partners. Australia: WHO statistical profile; 2015. Retrieved from: http://who.int/countries/aus/en/.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
