

Large Hip Impingement Area and Subspine Hip Impingement in Patients With Absolute Femoral Retroversion or Decreased Combined Version
- PMID: 36846812
- PMCID: PMC9950619
- DOI: 10.1177/23259671221148502
Large Hip Impingement Area and Subspine Hip Impingement in Patients With Absolute Femoral Retroversion or Decreased Combined Version
Abstract
Background: It remains unclear if femoral retroversion is a contraindication for hip arthroscopy in patients with femoroacetabular impingement (FAI).
Purpose: To compare the area and location of hip impingement at maximal flexion and during the FADIR test (flexion, adduction, internal rotation) in FAI hips with femoral retroversion, hips with decreased combined version, and asymptomatic controls.
Study design: Cross-sectional study; Level of evidence, 3.
Methods: Twenty-four symptomatic patients (37 hips) with anterior FAI were evaluated. All patients had femoral version (FV) <5° according to the Murphy method. Two subgroups were analyzed: 13 hips with absolute femoral retroversion (FV <0°) and 29 hips with decreased combined version (McKibbin index <20°). All patients were symptomatic and had anterior groin pain and a positive anterior impingement test ; all had undergone pelvic computed tomography (CT) scans to measure FV. The asymptomatic control group consisted of 26 hips. Dynamic impingement simulation of maximal flexion and FADIR test at 90° of flexion was performed with patient-specific CT-based 3-dimensional models. Extra- or intra-articular hip impingement area and location were compared between the subgroups and with control hips using nonparametric tests.
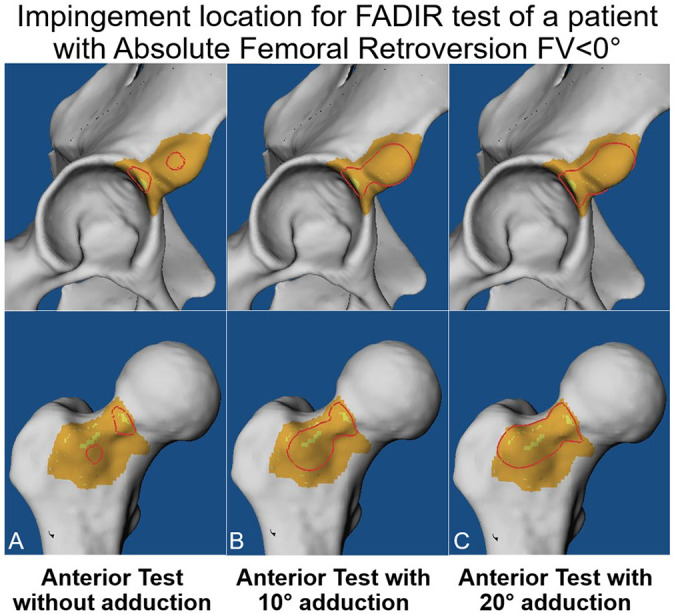
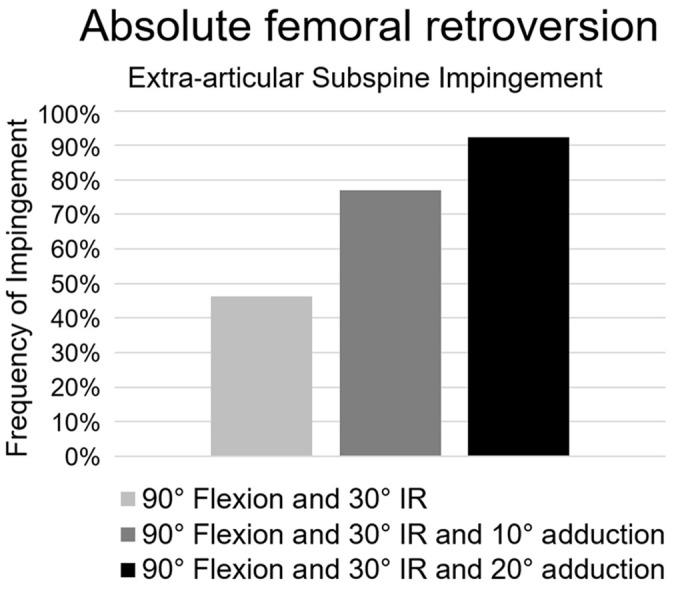
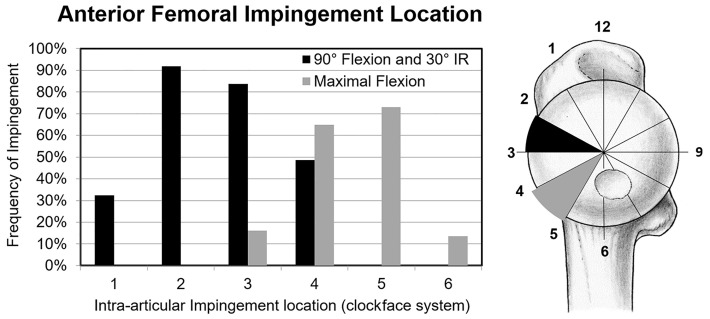
Results: Impingement area was significantly larger for hips with decreased combined version (<20°) versus combined version (≥20°) (mean ± SD; 171 ± 140 vs 78 ± 55 mm2; P = .012) and was significantly larger for hips with FV <0° (absolute femoral retroversion) vs FV >0° (P = .025). Hips with absolute femoral retroversion had a significantly higher frequency of extra-articular subspine impingement versus controls (92% vs 0%; P < .001), compared to 84% of patients with decreased combined version. Intra-articular femoral impingement location was most often (95%) anterosuperior and anterior (2-3 o'clock). Anteroinferior femoral impingement location was significantly different at maximal flexion (anteroinferior [4-5 o'clock]) versus the FADIR test (anterosuperior and anterior [2-3 o'clock]) (P < .001).
Conclusion: Patients with absolute femoral retroversion (FV <0°) had a larger hip impingement area, and most exhibited extra-articular subspine impingement. Preoperative FV assessment with advanced imaging (CT/magnetic resonance imaging) could help to identify these patients (without 3-dimensional modeling). Femoral impingement was located anteroinferiorly at maximal flexion and anterosuperiorly and anteriorly during the FADIR test.
Keywords: femoral retroversion; femoral version; femoroacetabular impingement; hip; hip arthroscopy; hip preservation surgery.
© The Author(s) 2023.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was provided from the Swiss National Science Foundation (grant P2BEP3_195241 to T.D.L.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures

Similar articles
-
Femoroacetabular Impingement Patients With Decreased Femoral Version Have Different Impingement Locations and Intra- and Extraarticular Anterior Subspine FAI on 3D-CT-Based Impingement Simulation: Implications for Hip Arthroscopy.Am J Sports Med. 2019 Nov;47(13):3120-3132. doi: 10.1177/0363546519873666. Epub 2019 Sep 20. Am J Sports Med. 2019. PMID: 31539275
-
Hip Impingement Location in Maximal Hip Flexion in Patients With Femoroacetabular Impingement With and Without Femoral Retroversion.Am J Sports Med. 2022 Sep;50(11):2989-2997. doi: 10.1177/03635465221110887. Epub 2022 Aug 29. Am J Sports Med. 2022. PMID: 36037094
-
Femoral impingement in maximal hip flexion is anterior-inferior distal to the cam deformity in femoroacetabular impingement patients with femoral retroversion : implications for hip arthroscopy.Bone Joint Res. 2023 Jan;12(1):22-32. doi: 10.1302/2046-3758.121.BJR-2022-0263.R1. Bone Joint Res. 2023. PMID: 36620909 Free PMC article.
-
[Torsional deformities of the femur in patients with femoroacetabular impingement : Dynamic 3D impingement simulation can be helpful for the planning of surgical hip dislocation and hip arthroscopy].Orthopade. 2020 Jun;49(6):471-481. doi: 10.1007/s00132-019-03847-x. Orthopade. 2020. PMID: 31853580 Review. German.
-
Influence of Femoral Version on the Outcomes of Hip Arthroscopic Surgery for Femoroacetabular Impingement or Labral Tears: A Systematic Review and Meta-analysis.Orthop J Sports Med. 2021 Jun 10;9(6):23259671211009192. doi: 10.1177/23259671211009192. eCollection 2021 Jun. Orthop J Sports Med. 2021. PMID: 34179203 Free PMC article. Review.
Cited by
-
Femoral Anteversion Angle as a Predictor of Anterior Hip Labral Length in Patients With Femoroacetabular Impingement Syndrome.Orthop J Sports Med. 2024 Aug 29;12(8):23259671241265448. doi: 10.1177/23259671241265448. eCollection 2024 Aug. Orthop J Sports Med. 2024. PMID: 39221042 Free PMC article.
-
Change of force and lever arm of the hip abductors after subtrochanteric de-/rotational osteotomy.J Exp Orthop. 2025 Jun 5;12(2):e70274. doi: 10.1002/jeo2.70274. eCollection 2025 Apr. J Exp Orthop. 2025. PMID: 40476013 Free PMC article.
-
Cam Morphology and Sex-Based Differences in the Proximal Femur Anatomy of Collegiate Athletes Without Hip Pain: A 3-Dimensional Statistical Shape Modeling Analysis.Orthop J Sports Med. 2025 Feb 6;13(2):23259671241309604. doi: 10.1177/23259671241309604. eCollection 2025 Feb. Orthop J Sports Med. 2025. PMID: 39931634 Free PMC article.
-
What Is the Influence of Femoral Version on Size, Tear Location, and Tear Pattern of the Acetabular Labrum in Patients With FAI?Clin Orthop Relat Res. 2024 Sep 1;482(9):1582-1594. doi: 10.1097/CORR.0000000000002961. Epub 2024 Jan 16. Clin Orthop Relat Res. 2024. PMID: 38231022
-
Predicting Outcomes in Hip Arthroscopy for Femoroacetabular Impingement Syndrome.Curr Rev Musculoskelet Med. 2024 Mar;17(3):59-67. doi: 10.1007/s12178-023-09880-w. Epub 2024 Jan 6. Curr Rev Musculoskelet Med. 2024. PMID: 38182802 Free PMC article. Review.
References
-
- Bedi A, Dolan M, Hetsroni I, et al. Surgical treatment of femoroacetabular impingement improves hip kinematics: a computer-assisted model. Am J Sports Med. 2011;39(suppl):43S–49S. doi:10.1177/0363546511414635 - PubMed
-
- Bouma H, Hogervorst T, Audenaert E, van Kampen P. Combining femoral and acetabular parameters in femoroacetabular impingement: the omega surface. Med Biol Eng Comput. 2015;53(11):1239–1246. doi:10.1007/s11517-015-1392-6 - PubMed
-
- Breighner RE, Bogner EA, Lee SC, Koff MF, Potter HG. Evaluation of osseous morphology of the hip using zero echo time magnetic resonance imaging. Am J Sports Med. 2019;47(14):3460–3468. doi:10.1177/0363546519878170 - PubMed
LinkOut - more resources
Full Text Sources
