

The Reality of Commercial Payer-Negotiated Rates in Cleft Lip and Palate Repair
- PMID: 36847669
- PMCID: PMC11240862
- DOI: 10.1097/PRS.0000000000010329
The Reality of Commercial Payer-Negotiated Rates in Cleft Lip and Palate Repair
Abstract
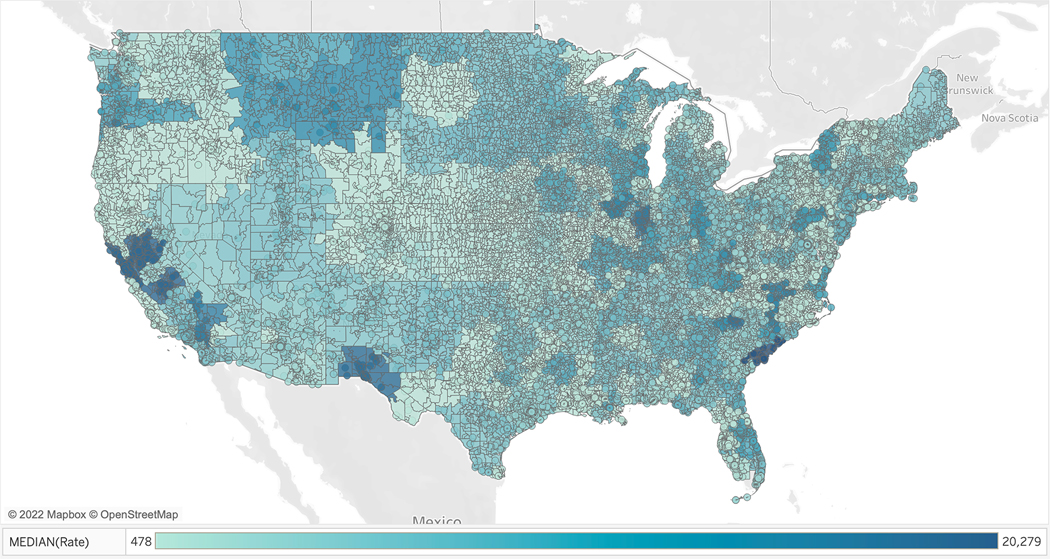
Background: Commercial payer-negotiated rates for cleft lip and palate surgery have not been evaluated on a national scale. The aim of this study was to characterize commercial rates for cleft care, both in terms of nationwide variation and in relation to Medicaid rates.
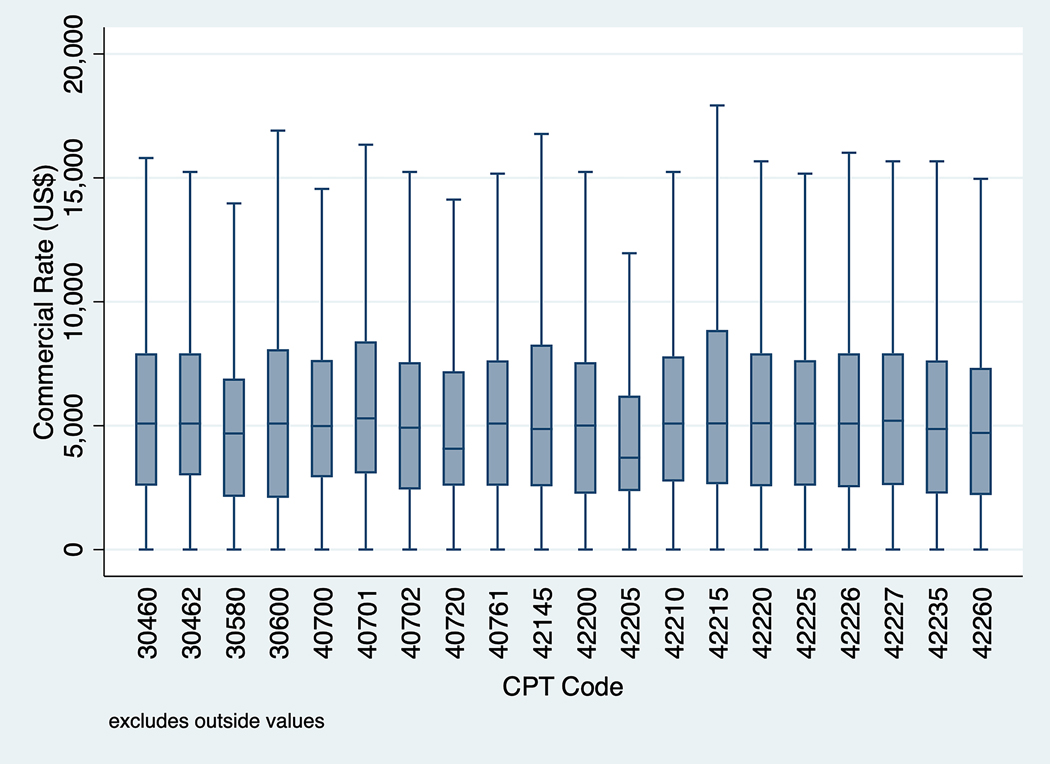
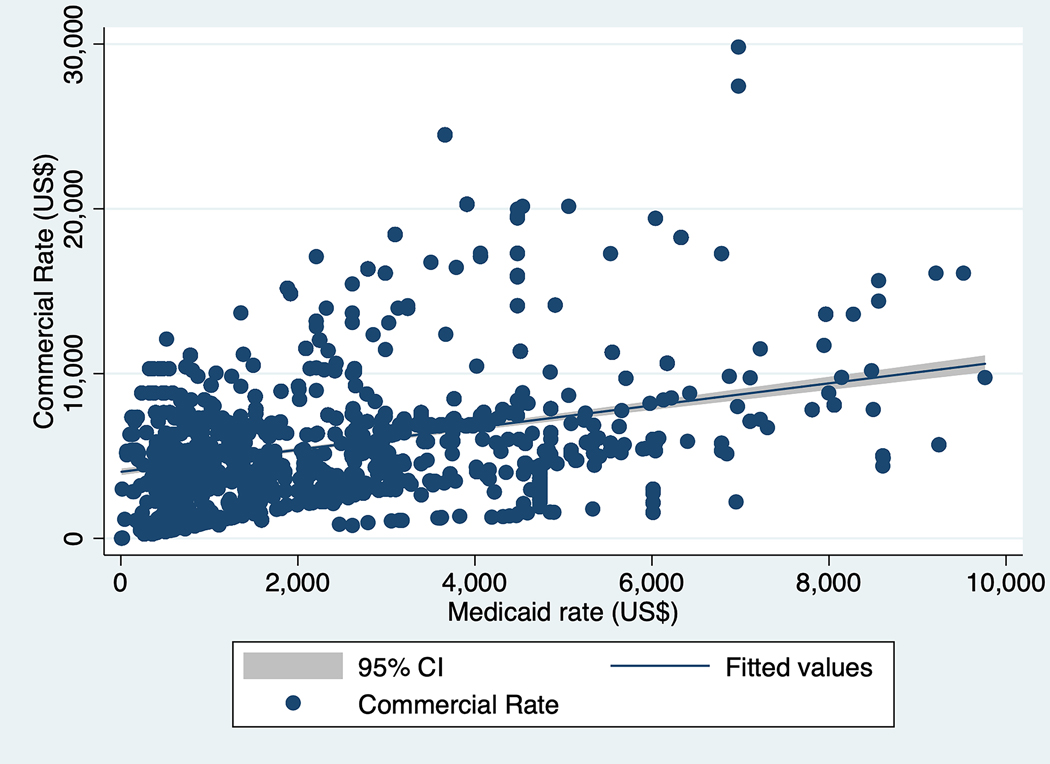
Methods: A cross-sectional analysis was performed of 2021 hospital pricing data from Turquoise Health, a data service platform that aggregates hospital price disclosures. The data were queried by CPT code to identify 20 cleft surgical services. Within- and across-hospital ratios were calculated per CPT code to quantify commercial rate variation. Generalized linear models were used to assess the relationship between median commercial rate and facility-level variables and between commercial and Medicaid rates.
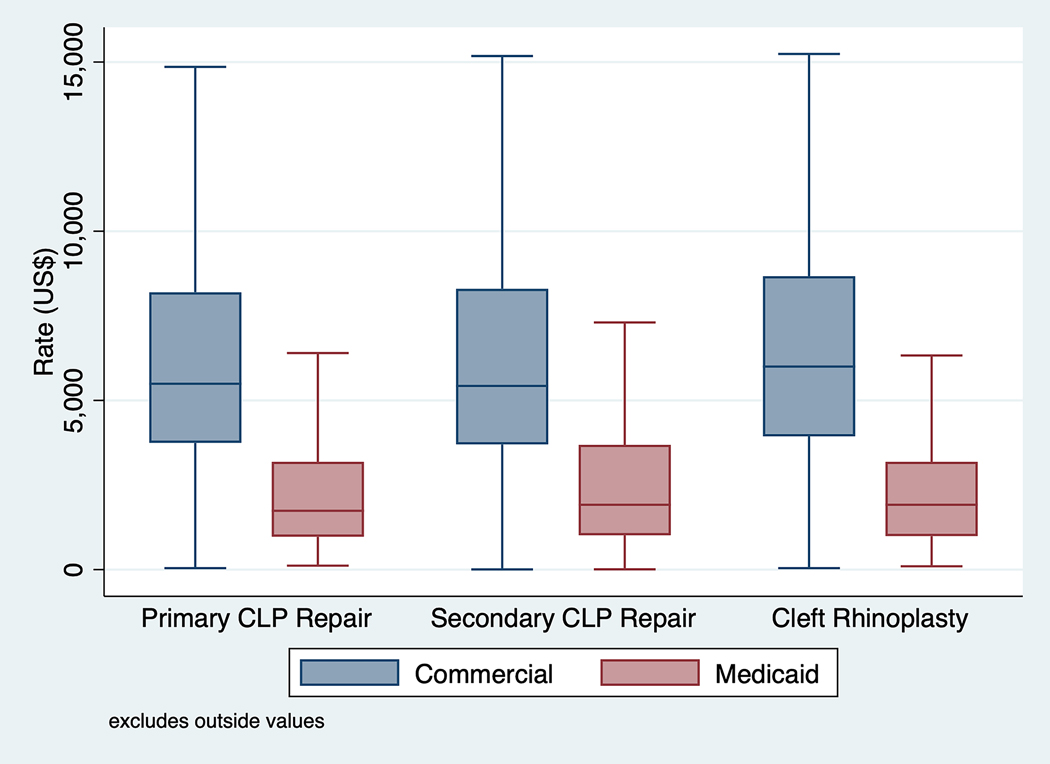
Results: There were 80,710 unique commercial rates from 792 hospitals. Within-hospital ratios for commercial rates ranged from 2.0 to 2.9 and across-hospital ratios ranged from 5.4 to 13.7. Median commercial rates per facility were higher than Medicaid rates for primary cleft lip and palate repair ($5492.20 versus $1739.00), secondary cleft lip and palate repair ($5429.10 versus $1917.00), and cleft rhinoplasty ($6001.00 versus $1917.00; P < 0.001). Lower commercial rates were associated with hospitals that were smaller ( P < 0.001), safety-net ( P < 0.001), and nonprofit ( P < 0.001). Medicaid rate was positively associated with commercial rate ( P < 0.001).
Conclusions: Commercial rates for cleft surgical care demonstrated marked variation within and across hospitals, and were lower for small, safety-net, or nonprofit hospitals. Lower Medicaid rates were not associated with higher commercial rates, suggesting that hospitals did not use cost-shifting to compensate for budget shortfalls resulting from poor Medicaid reimbursement.
Copyright © 2023 by the American Society of Plastic Surgeons.
Figures
Similar articles
-
Commercial Price Variation for Breast Reconstruction in the Era of Price Transparency.JAMA Surg. 2023 Feb 1;158(2):152-160. doi: 10.1001/jamasurg.2022.6402. JAMA Surg. 2023. PMID: 36515928 Free PMC article.
-
Out-of-Pocket Costs and Provider Payments in Cleft Lip and Palate Repair.Ann Plast Surg. 2022 May 1;88(4 Suppl 4):S343-S347. doi: 10.1097/SAP.0000000000003081. Epub 2022 Feb 21. Ann Plast Surg. 2022. PMID: 35180754 Free PMC article.
-
The financial impact of multidisciplinary cleft care: an analysis of hospital revenue to advance program development.Plast Reconstr Surg. 2013 Mar;131(3):615-622. doi: 10.1097/PRS.0b013e31827c6ffb. Plast Reconstr Surg. 2013. PMID: 23446572
-
How various surgical protocols of the unilateral cleft lip and palate influence the facial growth and possible orthodontic problems? Which is the best timing of lip, palate and alveolus repair? literature review.Stomatologija. 2014;16(2):53-60. Stomatologija. 2014. PMID: 25209227 Review.
-
Cleft Lip Repair, Nasoalveolar Molding, and Primary Cleft Rhinoplasty.Facial Plast Surg Clin North Am. 2016 Nov;24(4):453-466. doi: 10.1016/j.fsc.2016.06.015. Facial Plast Surg Clin North Am. 2016. PMID: 27712813 Review.
Cited by
-
Burn Care Funding in the Era of Price Transparency-Does Verification Signal Bargaining Power?J Burn Care Res. 2024 Sep 6;45(5):1117-1123. doi: 10.1093/jbcr/irae078. J Burn Care Res. 2024. PMID: 38733210 Free PMC article.
-
Commercial Insurance Rates and Coding for Lymphedema Procedures: The Current State of Confusion and Need for Consensus.Plast Reconstr Surg. 2024 Jan 1;153(1):245-255. doi: 10.1097/PRS.0000000000010591. Epub 2023 Apr 25. Plast Reconstr Surg. 2024. PMID: 37092977 Free PMC article.
-
Lower Commercial Rates for Breast Surgical Procedures are Associated with Socioeconomic Disadvantage: A Transparency in Coverage Analysis.Ann Surg Oncol. 2025 May;32(5):3695-3704. doi: 10.1245/s10434-024-16738-z. Epub 2024 Dec 24. Ann Surg Oncol. 2025. PMID: 39719512
-
Negotiated Rates for Surgical Cancer Care in the Era of Price Transparency-Prices Reflect Market Competition.Ann Surg. 2024 Mar 1;279(3):385-391. doi: 10.1097/SLA.0000000000006091. Epub 2023 Sep 4. Ann Surg. 2024. PMID: 37678179 Free PMC article.
References
-
- American Cleft Palate-Craniofacial Association. Paying for Treatment | ACPA Family Services. Published 2019. Accessed March 17, 2022. https://acpa-cpf.org/wp-content/uploads/2019/11/Paying-for-Treatment.pdf
-
- Committee on Child Health Financing, Racine AD, Long TF, et al. Children’s Health Insurance Program (CHIP): Accomplishments, Challenges, and Policy Recommendations. Pediatrics. 2014;133(3):e784–e793. - PubMed
-
- Deleyiannis FWB, TeBockhorst S, Castro DA. The Financial Impact of Multidisciplinary Cleft Care: An Analysis of Hospital Revenue to Advance Program Development. Plastic and Reconstructive Surgery. 2013;131(3):615–622. - PubMed
-
- Kaiser Family Foundation. Health Insurance Coverage of Children 0–18. KFF. Published October 23, 2020. Accessed March 16, 2022. https://www.kff.org/other/state-indicator/children-0-18/
-
- Kaura AS, Berlin NL, Momoh AO, Kozlow JH. State Variations in Public Payer Reimbursement for Common Plastic Surgery Procedures. Plastic and Reconstructive Surgery. 2018;142(6):1653–1661. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
