

Importance of intraoperative indocyanine green imaging in the management of non-occlusive mesenteric ischemia: a case report
- PMID: 36847887
- PMCID: PMC9971406
- DOI: 10.1186/s40792-023-01614-x
Importance of intraoperative indocyanine green imaging in the management of non-occlusive mesenteric ischemia: a case report
Abstract
Background: Non-obstructive intestinal ischemia (NOMI) is caused by intestinal vascular spasm and has a poor prognosis if not diagnosed and treated early. Indocyanine green (ICG) fluorescence imaging has been reported to be useful for the intraoperative assessment of the extent of intestinal resection required for NOMI. Few reports have described massive intestinal bleeding after conservative management of NOMI. We report a case of NOMI with massive postoperative bleeding from the site of an ICG contrast defect found before the initial surgery.
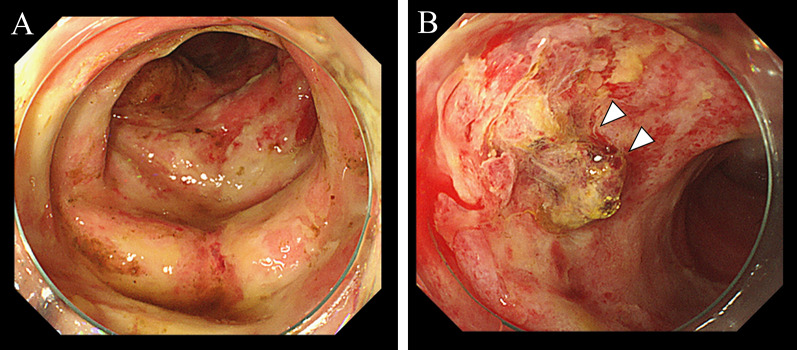
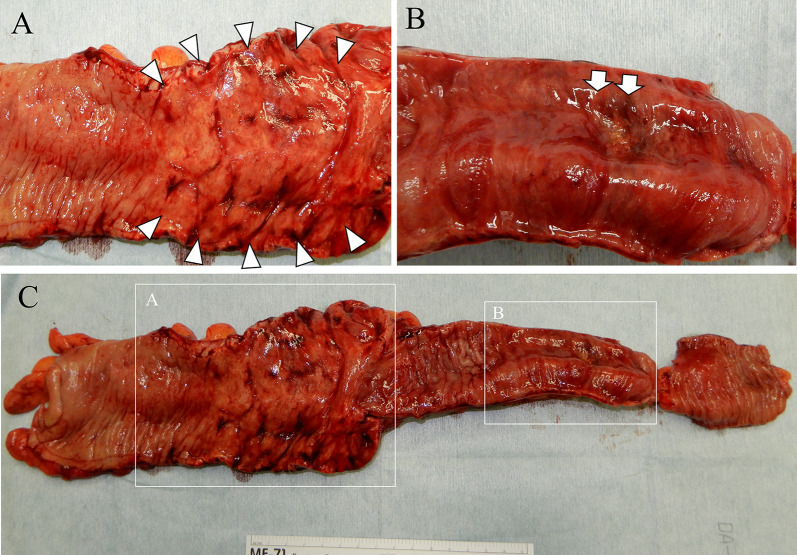
Case presentation: A 47-year-old woman with hemodialysis-dependent chronic kidney disease presented complaining of severe abdominal pain. A computed tomography scan showed portal gas and dilation of the small intestine, leading to a diagnosis of NOMI and subsequent emergency surgery. At the time of initial surgery, the contrast effect of ICG was slightly reduced, showing a granular distribution in the ascending colon to cecum (fine grain pattern) and significantly reduced in parts of the terminal ileum except around blood vessels (perivascular pattern). However, there was no obvious gross necrosis of the serosal surface, and the intestinal tract was not resected. The acute postoperative course was uneventful; however, the patient went into shock on the 24th postoperative day due to massive, small intestinal bleeding, and emergency surgery was performed. The bleeding originated from the section of the ileum that had complete loss of ICG contrast effect before the initial surgery. A right hemicolectomy with the terminal ileum resection was performed, and an ileo-transverse anastomosis was performed. The second post-operative course was uneventful.
Conclusions: We report a case of delayed hemorrhage of the ileum shown to have poor blood flow on ICG imaging at the initial surgery. Intraoperative ICG fluorescence imaging is useful in assessing the degree of intestinal ischemia for NOMI. When patients with NOMI are followed up without surgery, complications such as bleeding should be noted.
Keywords: Indocyanine green; Non-obstructive intestinal ischemia; Postoperative bleeding.
© 2023. The Author(s).
Conflict of interest statement
The authors report no declarations of interest.
Figures



Similar articles
-
Intraoperative indocyanine green fluorescence for precise resection of nonocclusive mesenteric ischemia: a case report and diagnostic considerations based on pathology findings.Surg Case Rep. 2024 Oct 4;10(1):230. doi: 10.1186/s40792-024-02024-3. Surg Case Rep. 2024. PMID: 39365410 Free PMC article.
-
Use of indocyanine green fluorescence imaging to determine the area of bowel resection in non-occlusive mesenteric ischemia: A case report.Int J Surg Case Rep. 2018;51:352-357. doi: 10.1016/j.ijscr.2018.09.024. Epub 2018 Sep 17. Int J Surg Case Rep. 2018. PMID: 30248629 Free PMC article.
-
Successful treatment of non-occlusive mesenteric ischemia (NOMI) using the HyperEye Medical System™ for intraoperative visualization of the mesenteric and bowel circulation: report of a case.Surg Today. 2014 Feb;44(2):359-62. doi: 10.1007/s00595-013-0503-y. Epub 2013 Feb 13. Surg Today. 2014. PMID: 23404392
-
Usefulness of indocyanine green fluorescence-guided small intestinal bleeding site identification in small bowel resection: a report of two cases and literature review.Clin J Gastroenterol. 2023 Jun;16(3):349-354. doi: 10.1007/s12328-023-01787-w. Epub 2023 Apr 12. Clin J Gastroenterol. 2023. PMID: 37046143 Review.
-
Non-occlusive mesenteric ischemia: two case reports and a short review of the literature.Acta Chir Belg. 2018 Dec;118(6):392-397. doi: 10.1080/00015458.2017.1408280. Epub 2017 Nov 25. Acta Chir Belg. 2018. PMID: 29173076 Review.
Cited by
-
Utility of indocyanine green fluorescent dye in emergency general surgery: a review of the contemporary literature.Front Surg. 2024 Feb 14;11:1345831. doi: 10.3389/fsurg.2024.1345831. eCollection 2024. Front Surg. 2024. PMID: 38419940 Free PMC article. Review.
-
Intraoperative indocyanine green fluorescence for precise resection of nonocclusive mesenteric ischemia: a case report and diagnostic considerations based on pathology findings.Surg Case Rep. 2024 Oct 4;10(1):230. doi: 10.1186/s40792-024-02024-3. Surg Case Rep. 2024. PMID: 39365410 Free PMC article.
-
Indocyanine green fluorescence-guided surgery in the emergency setting: the WSES international consensus position paper.World J Emerg Surg. 2025 Feb 13;20(1):13. doi: 10.1186/s13017-025-00575-w. World J Emerg Surg. 2025. PMID: 39948641 Free PMC article.
References
-
- Bulkley GB, Zuidema GD, Hamilton SR, O'Mara CS, Klacsmann PG, Horn SD. Intraoperative determination of small intestinal viability following ischemic injury: a prospective, controlled trial of two adjuvant methods (Doppler and fluorescein) compared with standard clinical judgment. Ann Surg. 1981;193:628–637. doi: 10.1097/00000658-198105000-00014. - DOI - PMC - PubMed
-
- Nitori N, Deguchi T, Kubota K, Yoshida M, Kato A, Kojima M, et al. Successful treatment of non-occlusive mesenteric ischemia (NOMI) using the HyperEye Medical System™ for intraoperative visualization of the mesenteric and bowel circulation: report of a case. Surg Today. 2014;44:359–362. doi: 10.1007/s00595-013-0503-y. - DOI - PubMed
LinkOut - more resources
Full Text Sources
