

Discrete Choice Experiment to Understand Japanese Patients' and Physicians' Preferences for Preventive Treatments for Migraine
- PMID: 36848008
- PMCID: PMC10043145
- DOI: 10.1007/s40120-023-00453-0
Discrete Choice Experiment to Understand Japanese Patients' and Physicians' Preferences for Preventive Treatments for Migraine
Abstract
Introduction: Self-injectable calcitonin gene-related peptide (CGRP) monoclonal antibody (mAb) auto-injectors and non-CGRP oral medications are currently available for migraine prevention in Japan. This study elicited the preferences for self-injectable CGRP mAbs and non-CGRP oral medications and determined differences in the relative importance of auto-injector attributes for patients and physicians in Japan.
Methods: Japanese adults with episodic (EM) or chronic (CM) migraine and physicians who treat migraine completed an online discrete choice experiment (DCE), asking participants to choose a hypothetical treatment they preferred between two self-injectable CGRP mAb auto-injectors and a non-CGRP oral medication. The treatments were described by seven treatment attributes, with attribute levels varying between questions. DCE data were analyzed using a random-constant logit model to estimate relative attribution importance (RAI) scores and predicted choice probabilities (PCP) of CGRP mAb profiles.
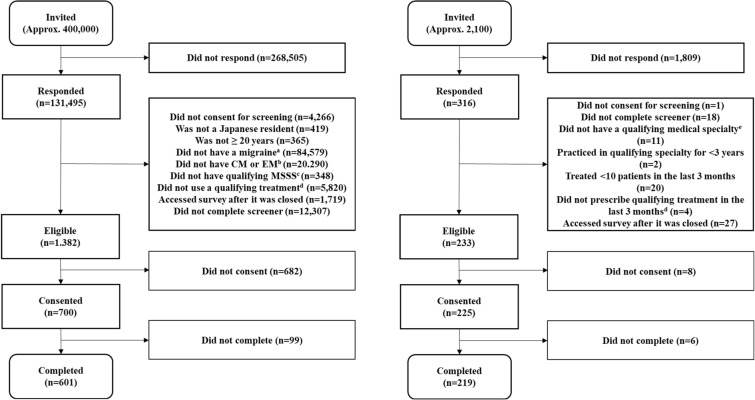
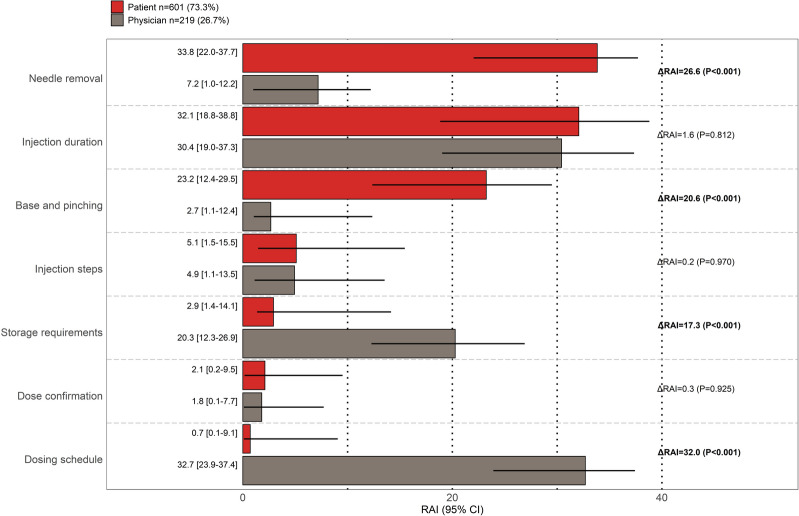
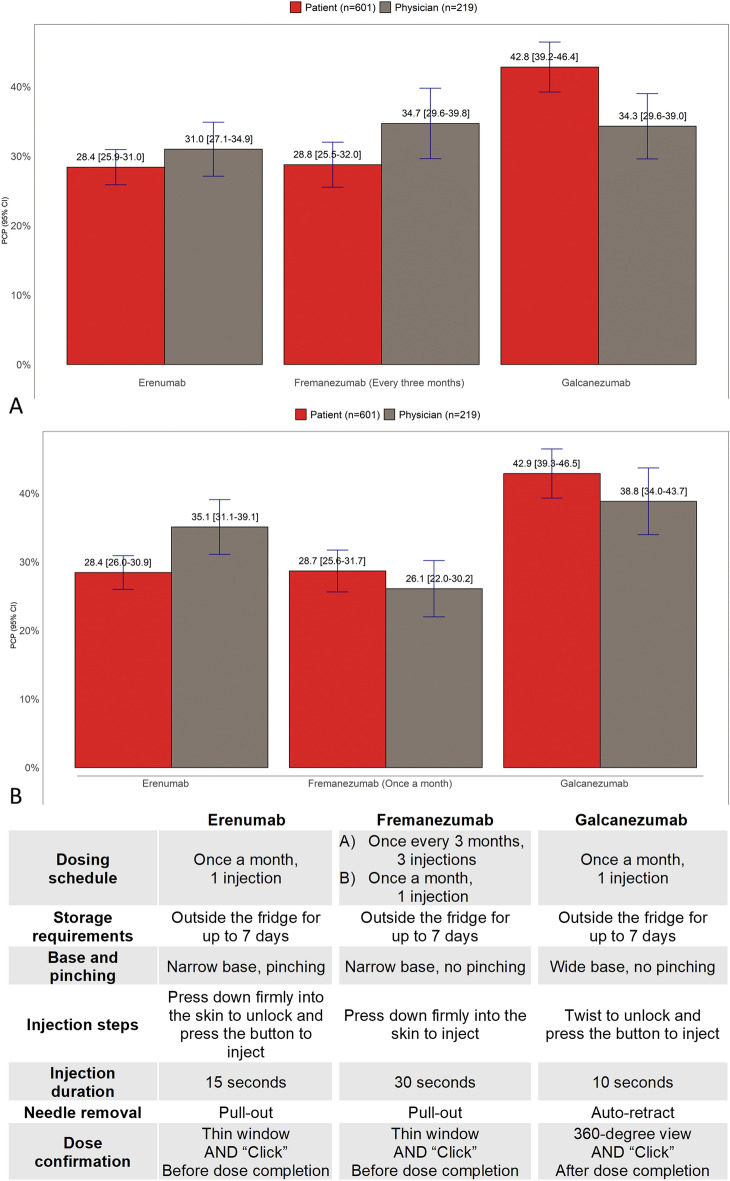
Results: A total of 601 patients (79.2% with EM, 60.1% female, mean age: 40.3 years) and 219 physicians (mean length of practice: 18.3 years) completed the DCE. About half (50.5%) of patients favored CGRP mAb auto-injectors, while others were skeptical of (20.2%) or averse (29.3%) to them. Patients most valued needle removal (RAI = 33.8%), shorter injection duration (RAI = 32.1%), and auto-injector base shape and need for skin pinching (RAI = 23.2%). Most physicians (87.8%) favored auto-injectors over non-CGRP oral medications. Physicians most valued less-frequent dosing RAI = 32.7%), shorter injection duration (30.4%), and longer storage outside the fridge (RAI = 20.3%). A profile comparable to galcanezumab showed a higher likelihood of being chosen by patients (PCP = 42.8%) than profiles comparable to erenumab (PCP = 28.4%) and fremanezumab (PCP = 28.8%). The PCPs of the three profiles were similar among physicians.
Conclusion: Many patients and physicians preferred CGRP mAb auto-injectors over non-CGRP oral medications and preferred a treatment profile similar to galcanezumab. Our results may encourage physicians in Japan to consider patient preferences when recommending migraine preventive treatments.
Keywords: CGRP monoclonal antibody; Discrete choice experiment; Migraine prevention; Patient and physician preferences.
© 2023. The Author(s).
Figures

Similar articles
-
A Discrete-Choice Experiment Assessing the Patient Preferences and Real-World Experiences of Patients with Migraine in Japan.Neurol Ther. 2024 Dec;13(6):1661-1683. doi: 10.1007/s40120-024-00663-0. Epub 2024 Sep 30. Neurol Ther. 2024. PMID: 39343868 Free PMC article.
-
Patient Preferences for Episodic Migraine Medications: A Discrete Choice Experiment of Self-Injectable Versus Oral Treatments Targeting Calcitonin Gene-Related Peptide Pathway.Patient Prefer Adherence. 2025 Mar 29;19:839-853. doi: 10.2147/PPA.S496736. eCollection 2025. Patient Prefer Adherence. 2025. PMID: 40177623 Free PMC article.
-
Patient Preferences for Self-Injectable Preventive Treatment for Migraine: A Multi-country Discrete Choice Experiment.Neurol Ther. 2025 Aug 2. doi: 10.1007/s40120-025-00801-2. Online ahead of print. Neurol Ther. 2025. PMID: 40753326
-
A stated preference survey to explore patient preferences for novel preventive migraine treatments.Headache. 2022 Oct;62(9):1187-1197. doi: 10.1111/head.14386. Epub 2022 Sep 1. Headache. 2022. PMID: 36047857 Free PMC article. Review.
-
Indirect Comparison of Topiramate and Monoclonal Antibodies Against CGRP or Its Receptor for the Prophylaxis of Episodic Migraine: A Systematic Review with Meta-Analysis.CNS Drugs. 2021 Aug;35(8):805-820. doi: 10.1007/s40263-021-00834-9. Epub 2021 Jul 16. CNS Drugs. 2021. PMID: 34272688 Free PMC article.
Cited by
-
A Discrete-Choice Experiment Assessing the Patient Preferences and Real-World Experiences of Patients with Migraine in Japan.Neurol Ther. 2024 Dec;13(6):1661-1683. doi: 10.1007/s40120-024-00663-0. Epub 2024 Sep 30. Neurol Ther. 2024. PMID: 39343868 Free PMC article.
-
A Systematic Literature Review of Preference Studies in Migraine Treatments.Patient. 2025 Sep 9. doi: 10.1007/s40271-025-00768-0. Online ahead of print. Patient. 2025. PMID: 40924386
-
Framing and Management of Migraines in Women: An Expert Opinion on Challenges, Current Approaches, and Future Multidisciplinary Perspectives.Healthcare (Basel). 2025 Jan 16;13(2):164. doi: 10.3390/healthcare13020164. Healthcare (Basel). 2025. PMID: 39857191 Free PMC article.
-
Patient Preferences for Episodic Migraine Medications: A Discrete Choice Experiment of Self-Injectable Versus Oral Treatments Targeting Calcitonin Gene-Related Peptide Pathway.Patient Prefer Adherence. 2025 Mar 29;19:839-853. doi: 10.2147/PPA.S496736. eCollection 2025. Patient Prefer Adherence. 2025. PMID: 40177623 Free PMC article.
-
The Evolving Landscape of Discrete Choice Experiments in Health Economics: A Systematic Review.Pharmacoeconomics. 2025 Aug;43(8):879-936. doi: 10.1007/s40273-025-01495-y. Epub 2025 May 21. Pharmacoeconomics. 2025. PMID: 40397369 Free PMC article.
References
-
- Hirata K, Ueda K, Komori M, et al. Comprehensive population-based survey of migraine in Japan: results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) study. Curr Med Res Opin. 2021;37(11):1945–1955. doi: 10.1080/03007995.2021.1971179. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
