

High- versus Low-Flow Extracorporeal Respiratory Support in Experimental Hypoxemic Acute Lung Injury
- PMID: 36848321
- PMCID: PMC10161753
- DOI: 10.1164/rccm.202212-2194OC
High- versus Low-Flow Extracorporeal Respiratory Support in Experimental Hypoxemic Acute Lung Injury
Abstract
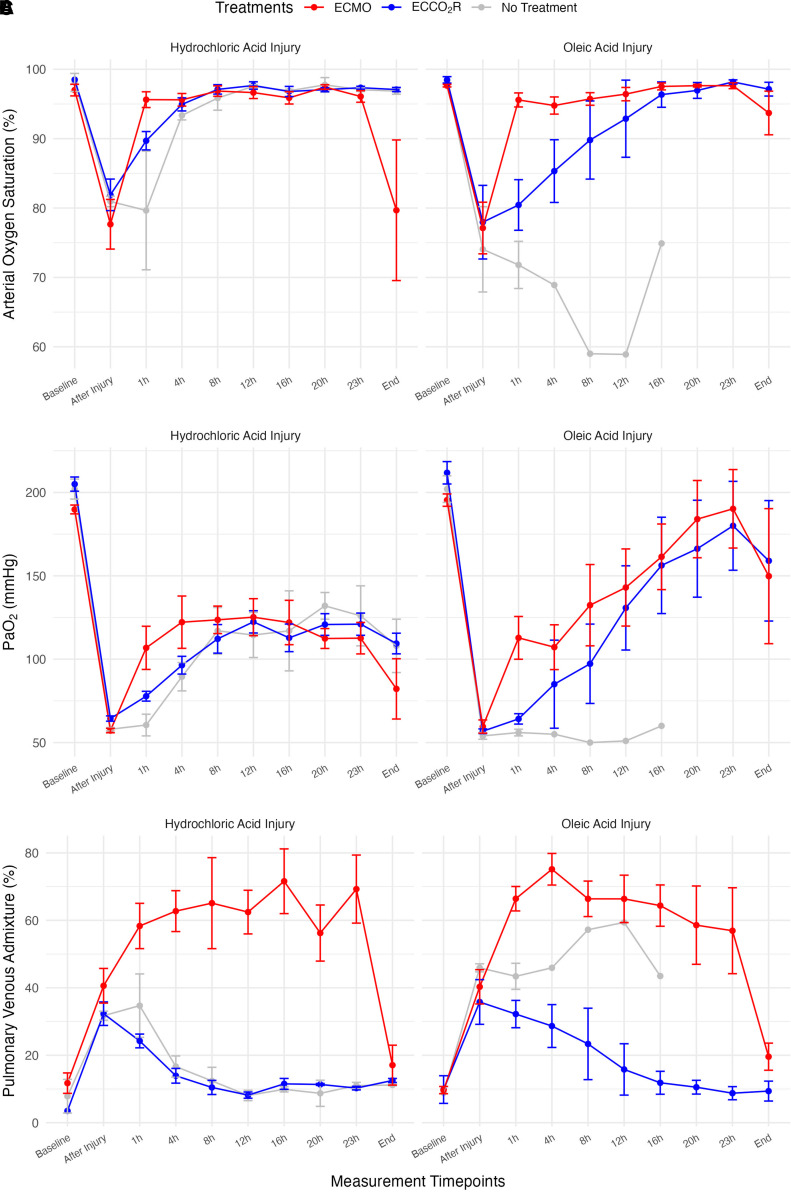
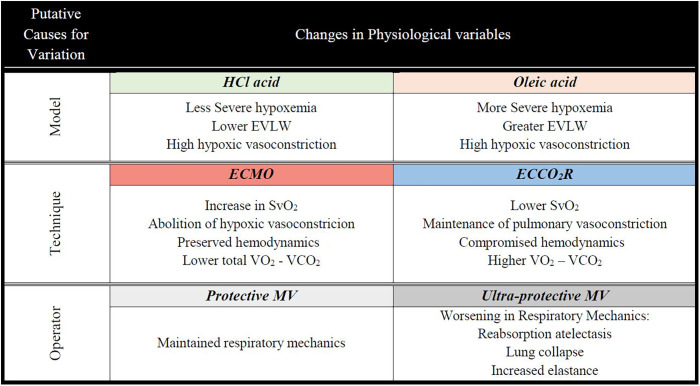
Rationale: In the EOLIA (ECMO to Rescue Lung Injury in Severe ARDS) trial, oxygenation was similar between intervention and conventional groups, whereas [Formula: see text]e was reduced in the intervention group. Comparable reductions in ventilation intensity are theoretically possible with low-flow extracorporeal CO2 removal (ECCO2R), provided oxygenation remains acceptable. Objectives: To compare the effects of ECCO2R and extracorporeal membrane oxygenation (ECMO) on gas exchange, respiratory mechanics, and hemodynamics in animal models of pulmonary (intratracheal hydrochloric acid) and extrapulmonary (intravenous oleic acid) lung injury. Methods: Twenty-four pigs with moderate to severe hypoxemia (PaO2:FiO2 ⩽ 150 mm Hg) were randomized to ECMO (blood flow 50-60 ml/kg/min), ECCO2R (0.4 L/min), or mechanical ventilation alone. Measurements and Main Results: [Formula: see text]o2, [Formula: see text]co2, gas exchange, hemodynamics, and respiratory mechanics were measured and are presented as 24-hour averages. Oleic acid versus hydrochloric acid showed higher extravascular lung water (1,424 ± 419 vs. 574 ± 195 ml; P < 0.001), worse oxygenation (PaO2:FiO2 = 125 ± 14 vs. 151 ± 11 mm Hg; P < 0.001), but better respiratory mechanics (plateau pressure 27 ± 4 vs. 30 ± 3 cm H2O; P = 0.017). Both models led to acute severe pulmonary hypertension. In both models, ECMO (3.7 ± 0.5 L/min), compared with ECCO2R (0.4 L/min), increased mixed venous oxygen saturation and oxygenation, and improved hemodynamics (cardiac output = 6.0 ± 1.4 vs. 5.2 ± 1.4 L/min; P = 0.003). [Formula: see text]o2 and [Formula: see text]co2, irrespective of lung injury model, were lower during ECMO, resulting in lower PaCO2 and [Formula: see text]e but worse respiratory elastance compared with ECCO2R (64 ± 27 vs. 40 ± 8 cm H2O/L; P < 0.001). Conclusions: ECMO was associated with better oxygenation, lower [Formula: see text]o2, and better hemodynamics. ECCO2R may offer a potential alternative to ECMO, but there are concerns regarding its effects on hemodynamics and pulmonary hypertension.
Keywords: [Formula: see text]O2; [Formula: see text]co2; acute respiratory distress syndrome; high-flow extracorporeal membrane oxygenation; low-flow extracorporeal CO2 removal.
Figures


Comment in
-
Lower Flow, Higher Costs? Recognizing Tradeoffs on the Spectrum of Extracorporeal Support for Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2023 May 1;207(9):1116-1118. doi: 10.1164/rccm.202303-0354ED. Am J Respir Crit Care Med. 2023. PMID: 36913243 Free PMC article. No abstract available.
-
Reply to Jha: Understanding the Pathophysiological and Clinical Changes in Lung Injury Models.Am J Respir Crit Care Med. 2023 Sep 1;208(5):633-634. doi: 10.1164/rccm.202305-0869LE. Am J Respir Crit Care Med. 2023. PMID: 37315321 Free PMC article. No abstract available.
-
Understanding the Pathophysiological and Clinical Changes in Lung Injury Models.Am J Respir Crit Care Med. 2023 Sep 1;208(5):632-633. doi: 10.1164/rccm.202305-0826LE. Am J Respir Crit Care Med. 2023. PMID: 37315324 Free PMC article. No abstract available.
References
-
- Hill JD, O’Brien TG, Murray JJ, Dontigny L, Bramson ML, Osborn JJ, et al. Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome): use of the Bramson membrane lung. N Engl J Med . 1972;286:629–634. - PubMed
-
- Zapol WM, Snider MT, Hill JD, Fallat RJ, Bartlett RH, Edmunds LH, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure: a randomized prospective study. JAMA . 1979;242:2193–2196. - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. CESAR Trial Collaboration Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet . 2009;374:1351–1363. - PubMed
-
- Davies A, Jones D, Bailey M, Beca J, Bellomo R, Blackwell N, et al. Australia, New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators Extracorporeal membrane oxygenation for 2009 influenza A(H1N1) acute respiratory distress syndrome. JAMA . 2009;302:1888–1895. - PubMed
-
- Combes A, Hajage D, Capellier G, Demoule A, Lavoué S, Guervilly C, et al. EOLIA Trial Group, REVA, and ECMONet Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med . 2018;378:1965–1975. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
