

Assessing the impact of community-based interventions on hypertension and diabetes management in three Minnesota communities: Findings from the prospective evaluation of US HealthRise programs
- PMID: 36848352
- PMCID: PMC9970068
- DOI: 10.1371/journal.pone.0279230
Assessing the impact of community-based interventions on hypertension and diabetes management in three Minnesota communities: Findings from the prospective evaluation of US HealthRise programs
Abstract
Background: Community-based health interventions are increasingly viewed as models of care that can bridge healthcare gaps experienced by underserved communities in the United States (US). With this study, we sought to assess the impact of such interventions, as implemented through the US HealthRise program, on hypertension and diabetes among underserved communities in Hennepin, Ramsey, and Rice Counties, Minnesota.
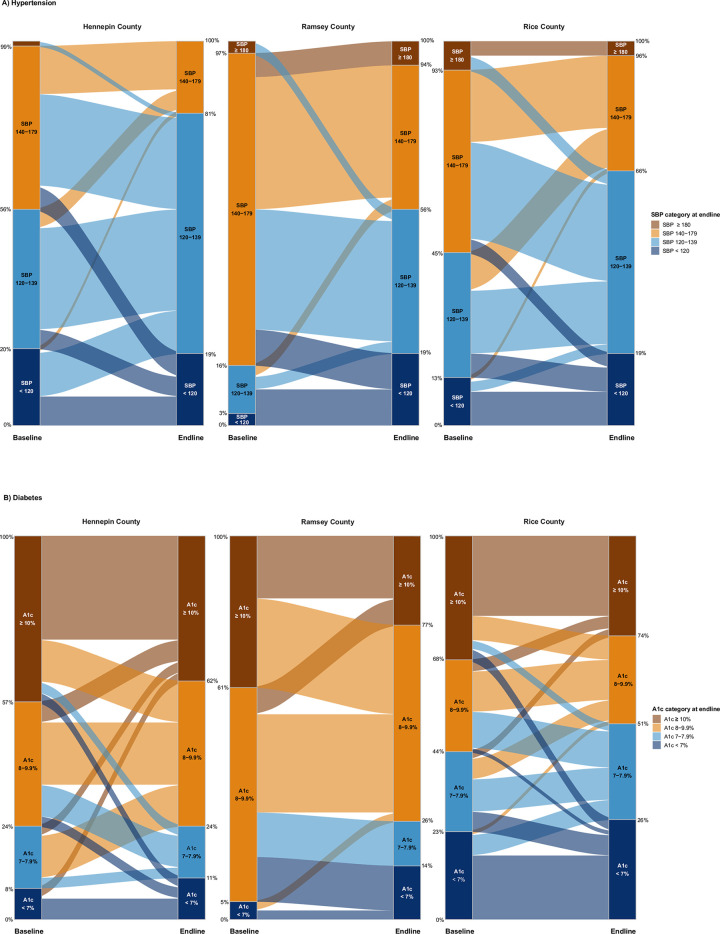
Methods and findings: HealthRise patient data from June 2016 to October 2018 were assessed relative to comparison patients in a difference-in-difference analysis, quantifying program impact on reducing systolic blood pressure (SBP) and hemoglobin A1c, as well as meeting clinical targets (< 140 mmHg for hypertension, < 8% Al1c for diabetes), beyond routine care. For hypertension, HealthRise participation was associated with SBP reductions in Rice (6.9 mmHg [95% confidence interval: 0.9-12.9]) and higher clinical target achievement in Hennepin (27.3 percentage-points [9.8-44.9]) and Rice (17.1 percentage-points [0.9 to 33.3]). For diabetes, HealthRise was associated with A1c decreases in Ramsey (1.3 [0.4-2.2]). Qualitative data showed the value of home visits alongside clinic-based services; however, challenges remained, including community health worker retention and program sustainability.
Conclusions: HealthRise participation had positive effects on improving hypertension and diabetes outcomes at some sites. While community-based health programs can help bridge healthcare gaps, they alone cannot fully address structural inequalities experienced by many underserved communities.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
PB and JD are employees of the Medtronic Foundation. CM, SM, NS, and TT are recipients of HealthRise grants from the Medtronic Foundation to implement HealthRise interventions. NF, KC, LSF, SW, MFB, JNC, DVC, RKG, KPH, CKJ, CRM, VM, BKP, MBR, BT, AW, and EG are recipients of funding from grants from the Medtronic Foundation to evaluate HealthRise interventions. There are no associated patents, products, or marketed products associated with this research. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- National Academies of Sciences E, Division H and M, Practice B on PH and PH, States C on C-BS to PHE in the U, Baciu A, Negussie Y, et al.. The State of Health Disparities in the United States. Communities in Action: Pathways to Health Equity. National Academies Press (US); 2017. Available: https://www.ncbi.nlm.nih.gov/books/NBK425844/ - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
