

Using real-time data to guide decision-making during an influenza pandemic: A modelling analysis
- PMID: 36848387
- PMCID: PMC9997955
- DOI: 10.1371/journal.pcbi.1010893
Using real-time data to guide decision-making during an influenza pandemic: A modelling analysis
Abstract
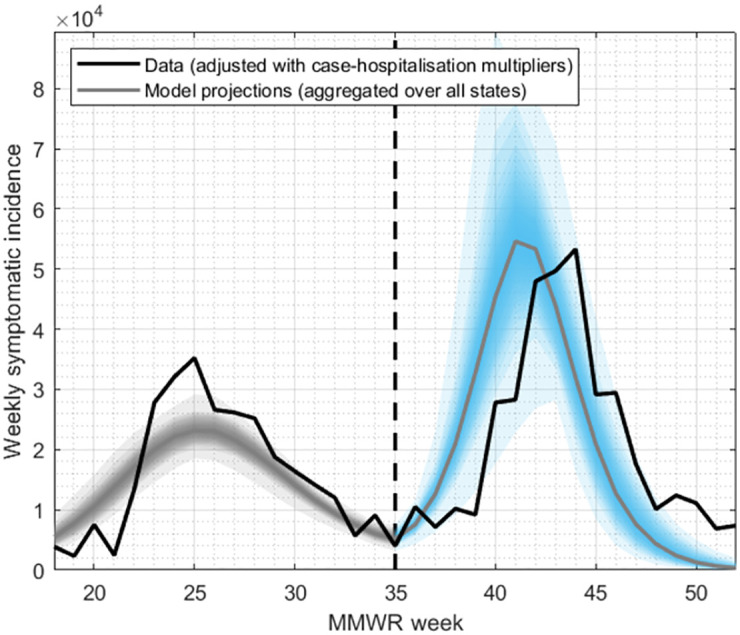
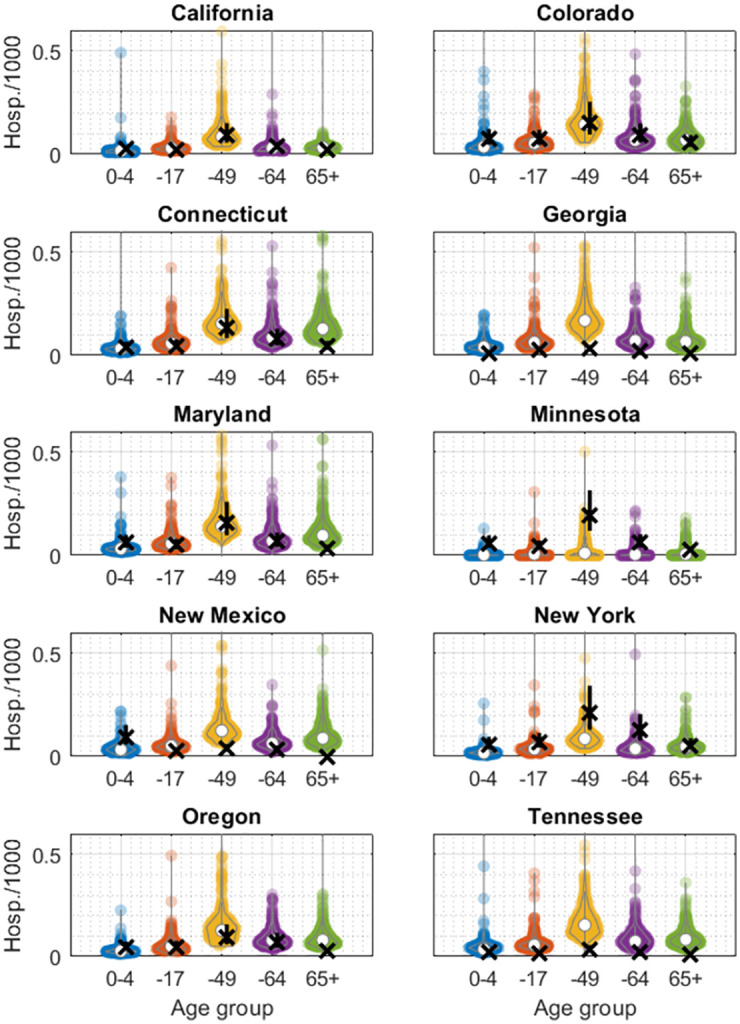
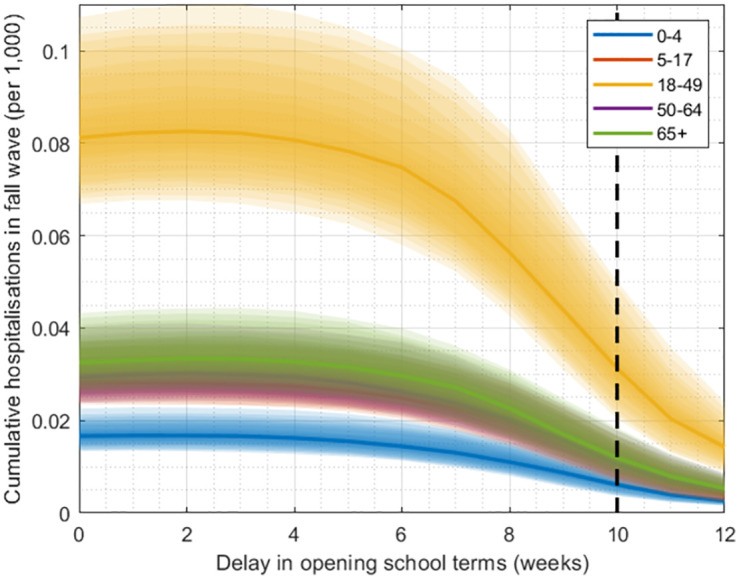
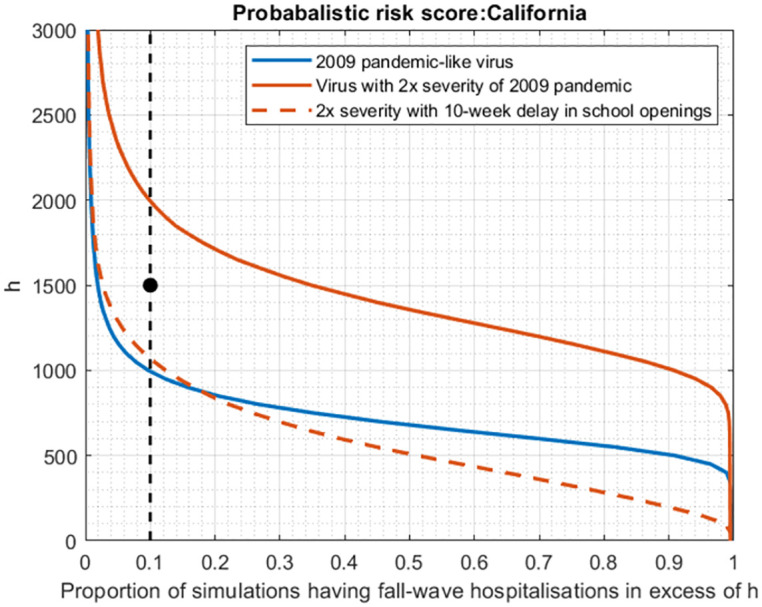
Influenza pandemics typically occur in multiple waves of infection, often associated with initial emergence of a novel virus, followed (in temperate regions) by a resurgence accompanying the onset of the annual influenza season. Here, we examined whether data collected from an initial pandemic wave could be informative, for the need to implement non-pharmaceutical measures in any resurgent wave. Drawing from the 2009 H1N1 pandemic in 10 states in the USA, we calibrated simple mathematical models of influenza transmission dynamics to data for laboratory confirmed hospitalisations during the initial 'spring' wave. We then projected pandemic outcomes (cumulative hospitalisations) during the fall wave, and compared these projections with data. Model results showed reasonable agreement for all states that reported a substantial number of cases in the spring wave. Using this model we propose a probabilistic decision framework that can be used to determine the need for preemptive measures such as postponing school openings, in advance of a fall wave. This work illustrates how model-based evidence synthesis, in real-time during an early pandemic wave, could be used to inform timely decisions for pandemic response.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
Authours have no competing interests to declare.
Figures

References
-
- Kucharski A, Mills H, Pinsent A, Fraser C, Van Kerkhove M, Donnelly C, et al.. Distinguishing Between Reservoir Exposure and Human-to-Human Transmission for Emerging Pathogens Using Case Onset Data. PLOS Currents Outbreaks. 2014. doi: 10.1371/currents.outbreaks.e1473d9bfc99d080ca242139a06c455f - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
