

Innate immune cell activation causes lung fibrosis in a humanized model of long COVID
- PMID: 36848564
- PMCID: PMC10013740
- DOI: 10.1073/pnas.2217199120
Innate immune cell activation causes lung fibrosis in a humanized model of long COVID
Abstract
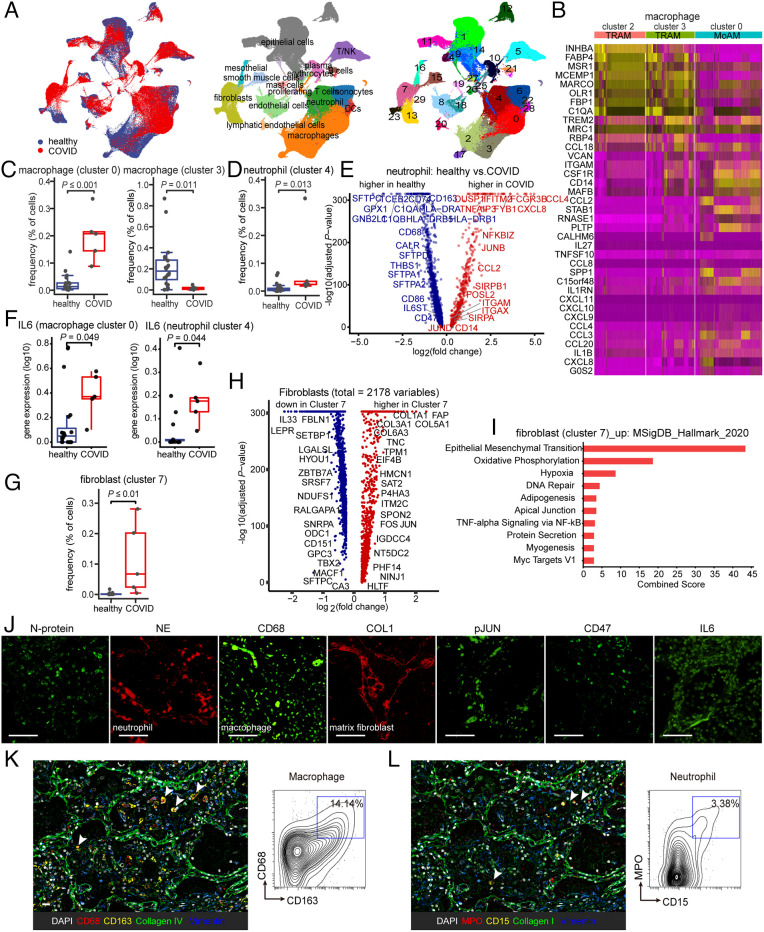
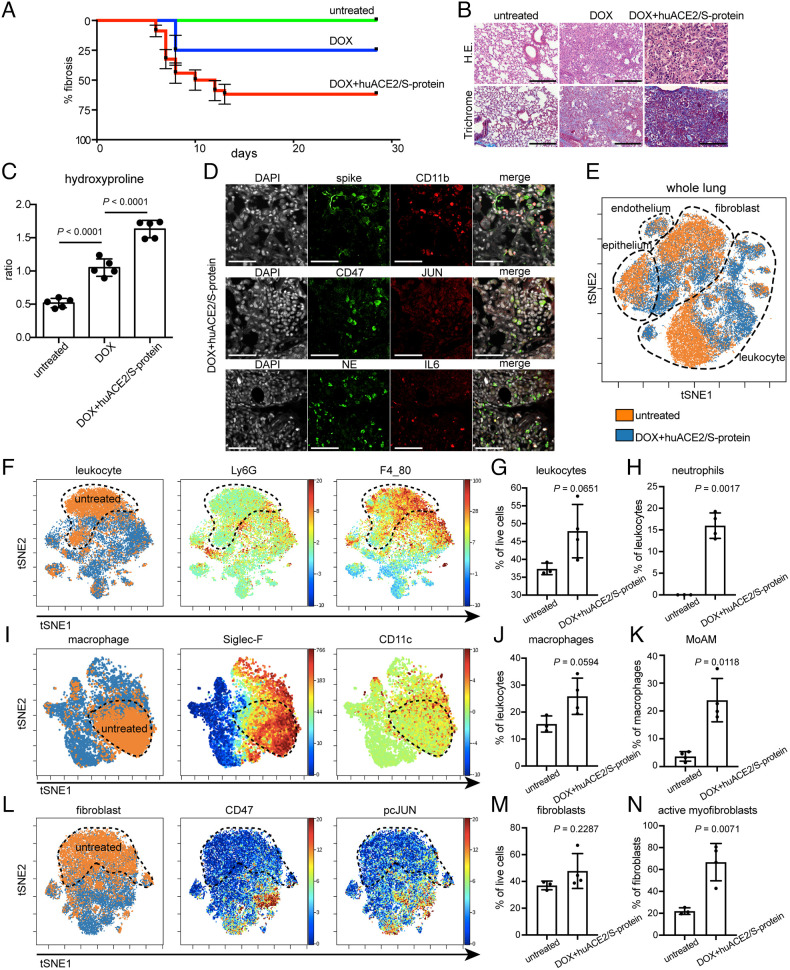
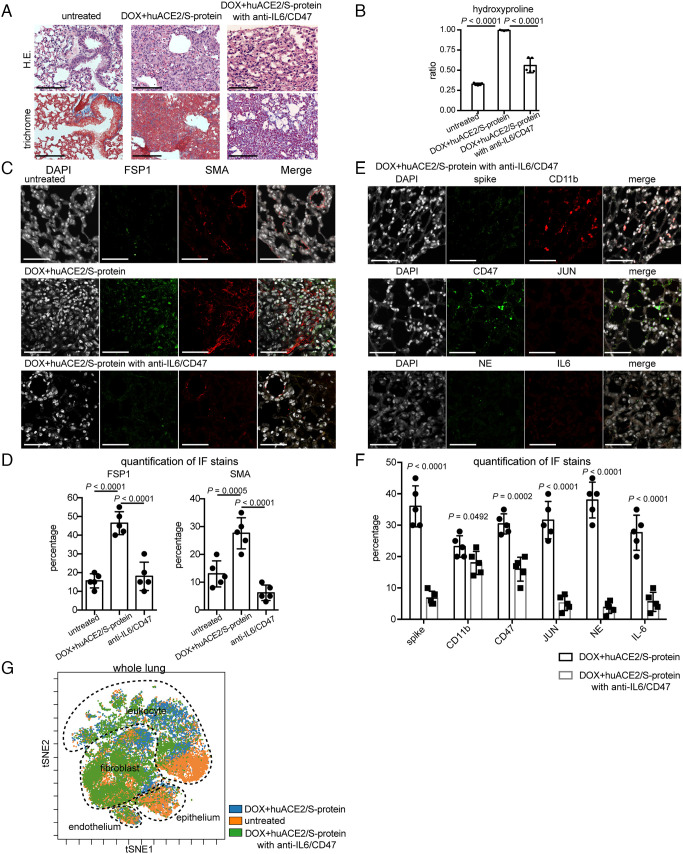
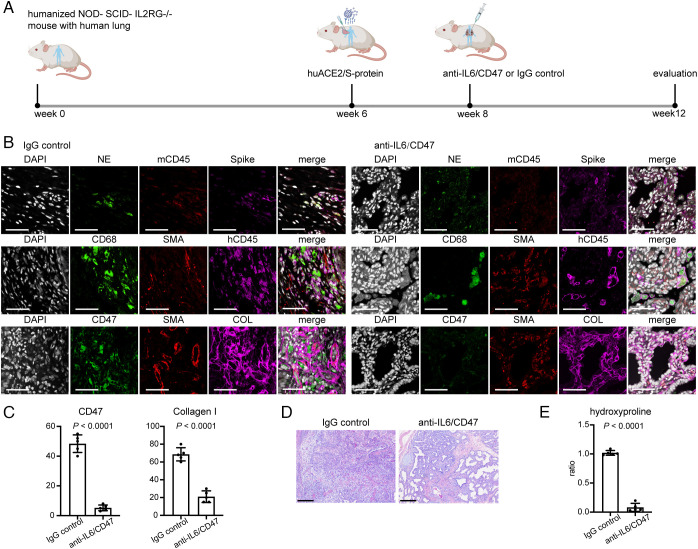
COVID-19 remains a global pandemic of an unprecedented magnitude with millions of people now developing "COVID lung fibrosis." Single-cell transcriptomics of lungs of patients with long COVID revealed a unique immune signature demonstrating the upregulation of key proinflammatory and innate immune effector genes CD47, IL-6, and JUN. We modeled the transition to lung fibrosis after COVID and profiled the immune response with single-cell mass cytometry in JUN mice. These studies revealed that COVID mediated chronic immune activation reminiscent to long COVID in humans. It was characterized by increased CD47, IL-6, and phospho-JUN (pJUN) expression which correlated with disease severity and pathogenic fibroblast populations. When we subsequently treated a humanized COVID lung fibrosis model by combined blockade of inflammation and fibrosis, we not only ameliorated fibrosis but also restored innate immune equilibrium indicating possible implications for clinical management of COVID lung fibrosis in patients.
Keywords: humanized mouse model; immune checkpoint therapy; innate immunity; long COVID pulmonary fibrosis.
Conflict of interest statement
The authors have patent filings to disclose: I.W. and G.W. have patents that have been licensed, and it is possible that they could receive royalties from them. No current consultation with companies in this field. I.W. is a founder and director of Bitterroot Bio, Inc, Pheast, Inc, and 48 Bio, Inc, none of which has programs in this field.
Figures
Comment in
-
Long COVID immune phenotypes identified for blockade.Nat Biotechnol. 2023 Apr;41(4):470. doi: 10.1038/s41587-023-01765-0. Nat Biotechnol. 2023. PMID: 37069391 No abstract available.
References
-
- Laing A. G., et al. , A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 26, 1623–1635 (2020). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
