

How to Treat Type B Aortic Dissections in the Presence of an Aberrant Right Subclavian Artery: A Systematic Review
- PMID: 36848908
- PMCID: PMC9970753
- DOI: 10.1055/s-0042-1757948
How to Treat Type B Aortic Dissections in the Presence of an Aberrant Right Subclavian Artery: A Systematic Review
Abstract
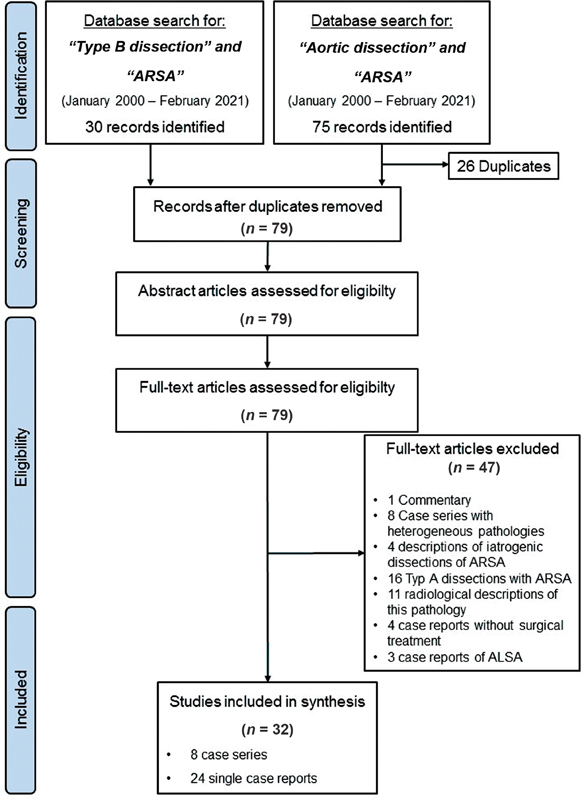
An aberrant right subclavian artery (ARSA) is the most common congenital variant of the aortic arch. Usually, this variation is largely asymptomatic, but sometimes it may be involved in aortic dissection (AD). Surgical management of this condition is challenging. The therapeutic options have been enriched in recent decades by establishing individualized endovascular or hybrid procedures. Whether these less invasive approaches bear advantages, and how they have changed the treatment of this rare pathology, is still unclear. Therefore, we conducted a systematic review. We performed a review of literature from the past 20 years (from January 2000 until February 2021) complying with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. All reported patients treated for Type B AD in the presence of an ARSA were identified and classified into three groups according to the received therapy (open, hybrid, and total endovascular). Patient characteristics, as well as in-hospital mortality, and major and minor complications were determined and statistically analyzed. We identified 32 relevant publications comprising 85 patients. Open arch repair has been offered to younger patients, but significantly less often in symptomatic patients needing urgent repair. Therefore, the maximum aortic diameter was also significantly larger in the open repair group compared with that in the hybrid or total endovascular repair group. Regarding the endpoints, we did not find significant differences. The literature review revealed that open surgical therapies are preferred in patients presenting with chronic dissections and larger aortic diameters, most likely because they are unsuitable for endovascular aortic repair. Hybrid and total endovascular approaches are more often applied in emergency situations, where aortic diameters remain smaller. All therapies demonstrated good, early, and midterm outcomes. But, these therapies carry potential risks in the long term. Therefore, long-term follow-up data are urgently needed to validate that these therapies are sustainable.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
The authors declare no conflict of interest related to this article.
Figures

References
-
- Abraham V, Mathew A, Cherian V, Chandran S, Mathew G. Aberrant subclavian artery: anatomical curiosity or clinical entity. Int J Surg. 2009;7(02):106–109. - PubMed
-
- Kouchoukos N T, Masetti P. Aberrant subclavian artery and Kommerell aneurysm: surgical treatment with a standard approach. J Thorac Cardiovasc Surg. 2007;133(04):888–892. - PubMed
-
- EACTS/ESVS scientific document group . Czerny M, Schmidli J, Adler S. Current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic surgery (EACTS) and the European Society for Vascular Surgery (ESVS) Eur J Cardiothorac Surg. 2019;55(01):133–162. - PubMed
-
- Guzman E D, Eagleton M J. Aortic dissection in the presence of an aberrant right subclavian artery. Ann Vasc Surg. 2012;26(06):8.6E15–8.6E20. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous