

Candidate mechanisms of acquired resistance to first-line osimertinib in EGFR-mutated advanced non-small cell lung cancer
- PMID: 36849494
- PMCID: PMC9971254
- DOI: 10.1038/s41467-023-35961-y
Candidate mechanisms of acquired resistance to first-line osimertinib in EGFR-mutated advanced non-small cell lung cancer
Erratum in
-
Author Correction: Candidate mechanisms of acquired resistance to first-line osimertinib in EGFR-mutated advanced non-small cell lung cancer.Nat Commun. 2023 Jun 1;14(1):3179. doi: 10.1038/s41467-023-38999-0. Nat Commun. 2023. PMID: 37263992 Free PMC article. No abstract available.
Abstract
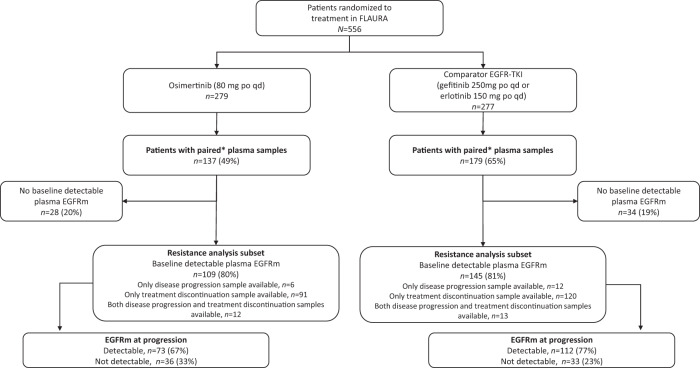
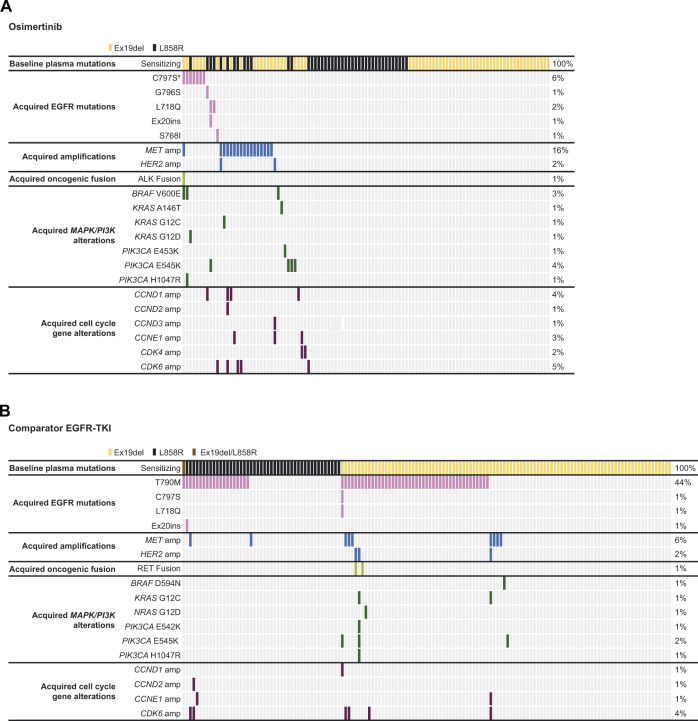
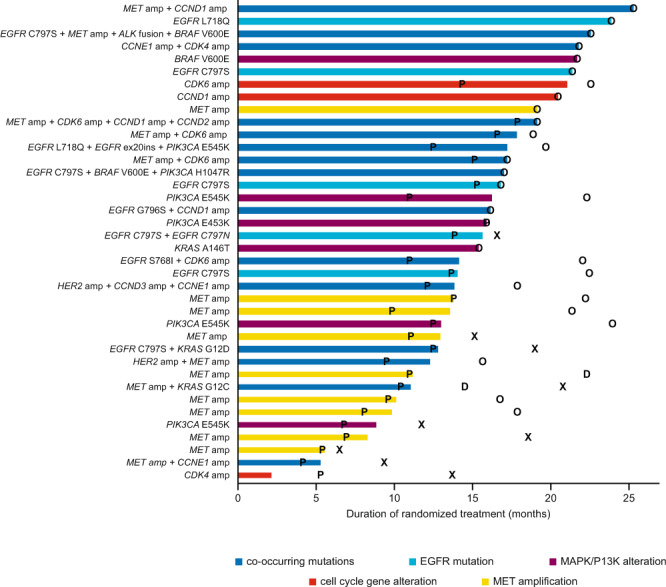
Osimertinib, an epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI), potently and selectively inhibits EGFR-TKI-sensitizing and EGFR T790M resistance mutations. In the Phase III FLAURA study (NCT02296125), first-line osimertinib improved outcomes vs comparator EGFR-TKIs in EGFRm advanced non-small cell lung cancer. This analysis identifies acquired resistance mechanisms to first-line osimertinib. Next-generation sequencing assesses circulating-tumor DNA from paired plasma samples (baseline and disease progression/treatment discontinuation) in patients with baseline EGFRm. No EGFR T790M-mediated acquired resistance are observed; most frequent resistance mechanisms are MET amplification (n = 17; 16%) and EGFR C797S mutations (n = 7; 6%). Future research investigating non-genetic acquired resistance mechanisms is warranted.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: J.C. reports employment and stock ownership with AstraZeneca. J.E.G. reports receiving honoraria from AstraZeneca, Genenech, Bristol-Myers Squibb, Takeda, EMD Serano Merck; and has received research grants/funding from AstraZeneca, Genentech, Bristol-Myers Squibb, BI, Takeda, Array, Merck. Y.C. reports no conflicts of interest. Y.O. reports undertaking an advisory role for AstraZeneca, Chugai, ONO, Bristol-Myers Squibb, Kyorin, Celltrion, Amgen, and Nippon Kayaku; reports receiving honoraria from AstraZeneca, Chugai, Eli Lilly, ONO, Bristol-Myers Squibb, Boehringer Ingelheim, Bayer, Pfizer, MSD, Taiho, Nippon Kayaku, and Kyowa Hakko Kirin; and has received grants or funds from AstraZeneca, Chugai, Lilly, ONO, BMS, Kyorin, Dainippon- Sumitomo, Pfizer, Taiho, Novartis, Kissei, Ignyta, Takeda, Kissei, Daiichi-Sankyo, Janssen, and LOXO. F.I. has received honoraria and research funding from AstraZeneca. B.C.C. reports stock ownership with TheraCanVac Inc, Gencurix Inc, Bridgebio therapeutics, KANAPH Therapeutic Inc, Cyrus Therapeutics, and Interpark Bio Convergence Corp; reports participating in an advisory role for KANAPH Therapeutic Inc, Brigebio Therapeutics, Cyrus Therapeutics, and Guardant Health; has received consulting fees from Novartis, AstraZeneca, Boehringer-Ingelheim, Roche, Bristol-Myers Squibb, ONO, Yuhan, Pfizer, Eli Lilly, Janssen, Takeda, MSD, Janssen, Medpacto, and Blueprint medicines; has received grants or funds from Novartis, Bayer, AstraZeneca, MOGAM Institute, Dong-A ST, Champions Oncology, Janssen, Yuhan, ONO, Dizal Pharma, MSD, Abbvie, Medpacto, GI Innovation, Eli Lilly, Blueprint medicines, and Interpark Bio Convergence Corp; has received royalties from Campions Oncology; and is the founder of DAAN Biotherapeutics. M-C.L. is on the board of directors for AstraZeneca and Boehringer Ingelheim, has received honoraria from Roche; and has received consulting fees from AstraZeneca, Boehringer Ingelheim and MSD. M.M. has received honoraria from Bristol-Myers Squibb, MSD, Boehringer Ingelheim, AstraZeneca, Roche, Kyowa Kyrin, Pierre Fabre, Takeda, Bayer and has received research funding from Bristol-Myers Squibb. R.S. reports employment with the Maidstone and Tunbridge Wells NHS Trust; participated in an advisory role for AstraZeneca, Roche, Pfizer and Boehringer Ingelheim; and has received honoraria from AstraZeneca, Roche, Pfizer, and Boehringer Ingelheim. Y.R. reports employment and stock ownership with AstraZeneca. A.T. reports employment and stock ownership with AstraZeneca. A.M. reports employment and stock ownership with AstraZeneca. J.C.B. reports employment and stock ownership with AstraZeneca. R.J.H. reports employment and stock ownership with AstraZeneca. S.S.R. has participated in an advisory role for Amgen, AstraZeneca, Bristol-Myers Squibb, Genentech, Merck, Tesaro, Takeda, GlaxoSmithKline, Daichii Sankyo, and Eisai; is on the board of directors for the International Association for Study of Lung Cancer; has received consulting fees from Amgen, AstraZeneca, Bristol-Myers Squibb, Genentech, Merck, Tesaro, Takeda, GlaxoSmithKline, Daichii Sankyo, and Eisai; and has received grants or funds from Amgen, Advaxis, AstraZeneca, BMS, Merck, Tesaro, Takeda, and Genmab.
Figures
References
-
- Planchard, D. et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. †Updated version published 15 September 2020 by the ESMO Guidelines Committee. 25 September
-
- Kuiper JL, et al. Incidence of T790M mutation in (sequential) rebiopsies in EGFR-mutated NSCLC-patients. Lung Cancer. 2014;85:19–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
