

Changes in preterm birth and stillbirth during COVID-19 lockdowns in 26 countries
- PMID: 36849590
- PMCID: PMC10129868
- DOI: 10.1038/s41562-023-01522-y
Changes in preterm birth and stillbirth during COVID-19 lockdowns in 26 countries
Abstract
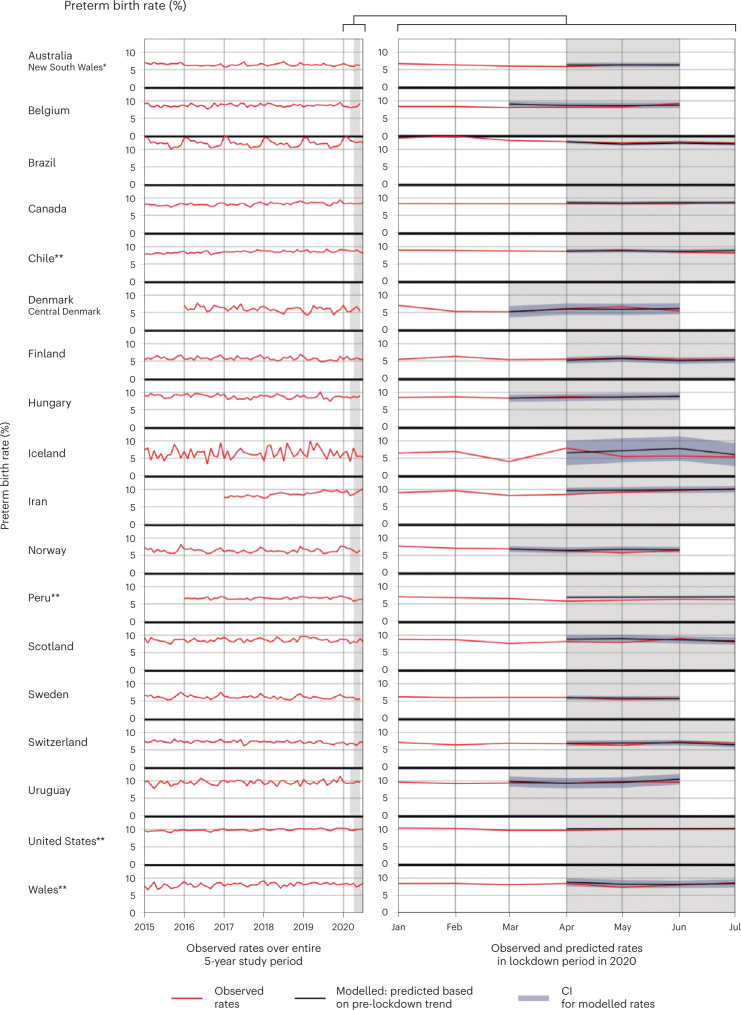
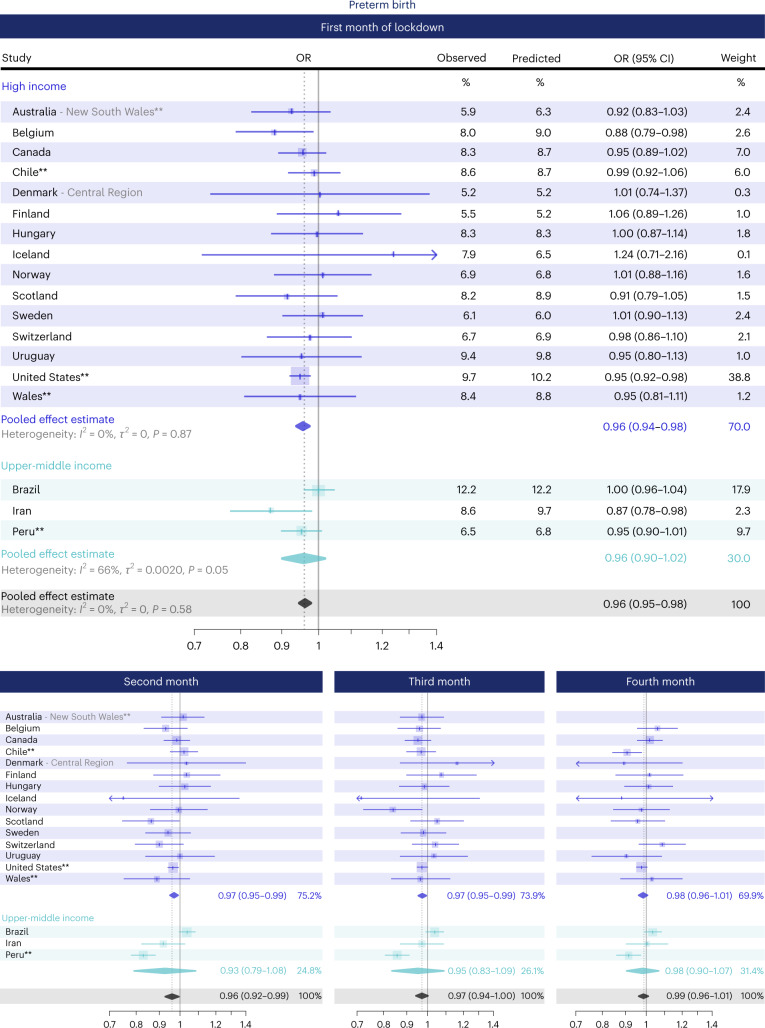
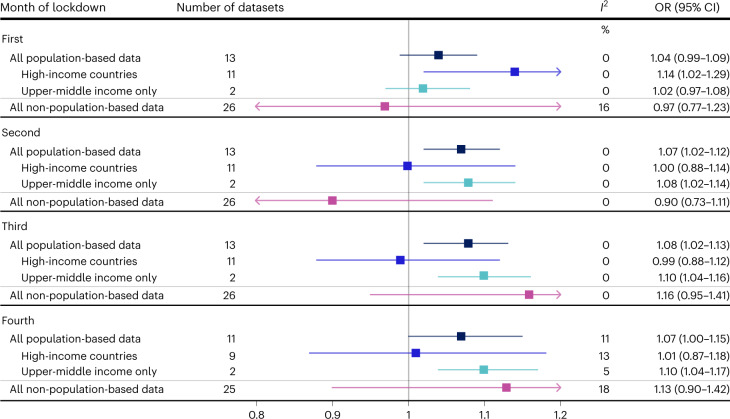
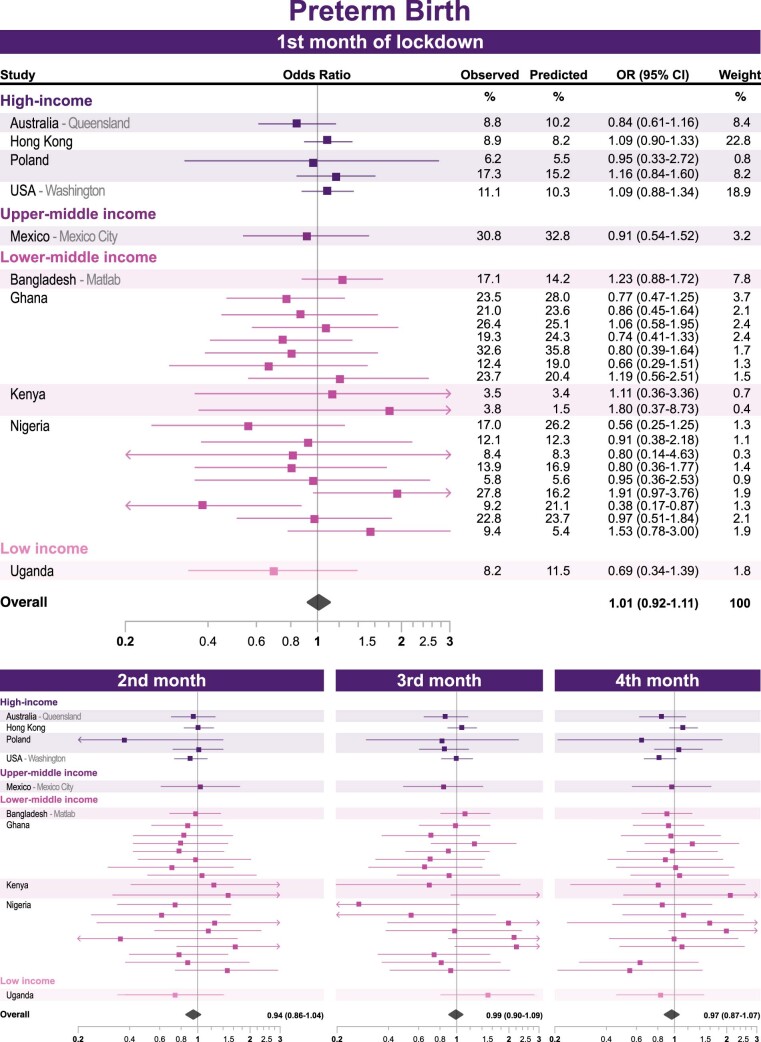
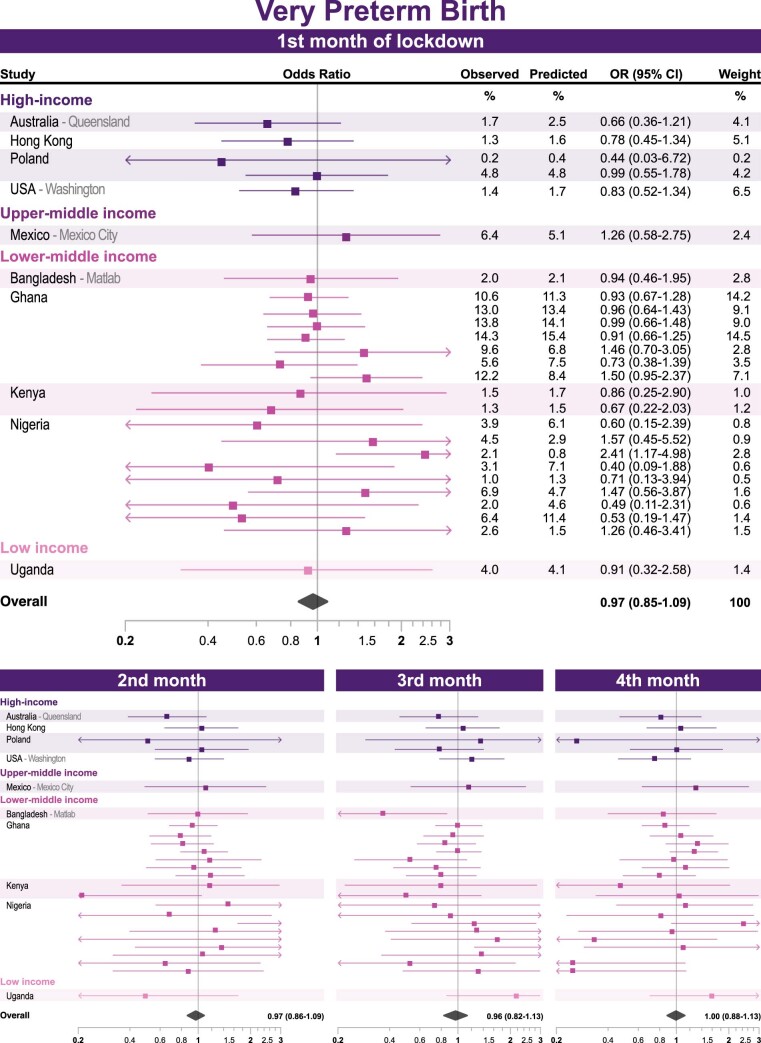
Preterm birth (PTB) is the leading cause of infant mortality worldwide. Changes in PTB rates, ranging from -90% to +30%, were reported in many countries following early COVID-19 pandemic response measures ('lockdowns'). It is unclear whether this variation reflects real differences in lockdown impacts, or perhaps differences in stillbirth rates and/or study designs. Here we present interrupted time series and meta-analyses using harmonized data from 52 million births in 26 countries, 18 of which had representative population-based data, with overall PTB rates ranging from 6% to 12% and stillbirth ranging from 2.5 to 10.5 per 1,000 births. We show small reductions in PTB in the first (odds ratio 0.96, 95% confidence interval 0.95-0.98, P value <0.0001), second (0.96, 0.92-0.99, 0.03) and third (0.97, 0.94-1.00, 0.09) months of lockdown, but not in the fourth month of lockdown (0.99, 0.96-1.01, 0.34), although there were some between-country differences after the first month. For high-income countries in this study, we did not observe an association between lockdown and stillbirths in the second (1.00, 0.88-1.14, 0.98), third (0.99, 0.88-1.12, 0.89) and fourth (1.01, 0.87-1.18, 0.86) months of lockdown, although we have imprecise estimates due to stillbirths being a relatively rare event. We did, however, find evidence of increased risk of stillbirth in the first month of lockdown in high-income countries (1.14, 1.02-1.29, 0.02) and, in Brazil, we found evidence for an association between lockdown and stillbirth in the second (1.09, 1.03-1.15, 0.002), third (1.10, 1.03-1.17, 0.003) and fourth (1.12, 1.05-1.19, <0.001) months of lockdown. With an estimated 14.8 million PTB annually worldwide, the modest reductions observed during early pandemic lockdowns translate into large numbers of PTB averted globally and warrant further research into causal pathways.
© 2023. The Author(s).
Conflict of interest statement
M.B.A. holds a Tier 2 Canada Research Chair in the Developmental Origins of Chronic Disease at the University of Manitoba and is a Fellow in the Canadian Institutes for Advanced Research (CIFAR) Humans and the Microbiome Program. Her effort on this project was partly supported by HDR UK and ICODA. K.K.C.M. declares support from The Innovation and Technology Commission of the Hong Kong Special Administrative Region Government, and Hong Kong Research Grants Council Collaborative Research Fund Coronavirus Disease (COVID-19) and Novel Infectious Disease Research Exercise (Ref: C7154-20G) and grants from C W Maplethorpe Fellowship, National Institute of Health Research UK, European Commission Framework Horizon 2020 and has consulted for IQVIA Ltd. A.S. is supported by ICODA and HDR UK, and has received a research grant from HDR UK to the BREATHE Hub. He participates on the Scottish and UK Government COVID-19 Advisory Committees, unremunerated. S.J.S. is supported by a Wellcome Trust Clinical Career Development Fellowship (209560/Z/17/Z) and HDR UK, and has received personal fees from Hologic and Natera outside the submitted work. D.B. is supported by a National Health and Medical Research Council (Australia) Investigator Grant (GTN1175744). I.C.K.W. declares support from The Innovation and Technology Commission of the Hong Kong Special Administrative Region Government, and Hong Kong Research Grants Council Collaborative Research Fund Coronavirus Disease (COVID-19) and Novel Infectious Disease Research Exercise (Ref: C7154-20G), and grants from Hong Kong Research Grant Council, National Institute of Health Research UK, and European Commission Framework Horizon 2020. H.Z. is supported by a UNSW Scientia Program Award and reports grants from European Commission Framework Horizon 2020, Icelandic Centre for Research, and Australia’s National Health and Medical Research Council. H.Z. was an employee of the UNSW Centre for Big Data Research in Health, which received funding from AbbVie Australia to conduct research, unrelated to the current study. I.I.A.A., C.D.A., K.A., A.I.A., L.C., S.S., G.E.-G., O.W.G., L. Huicho, S.H., A.K., K.L., V.N., I.P., N.R.R., T.R., T.A.H.R., V.L.S., E.M.S., L.T., R.W. and H.Z. received funding from HDRUK (grant #2020.106) to support data collection for the iPOP study. K.H., R.B., S.O.E., A.R.-P. and J.H. receive salary from ICODA. M.B. received trainee funding from HDRUK (grant #2020.106). J.E.M. received trainee funding from HDRUK (grant #2020.109). Other relevant funding awarded to authors to conduct research for iPOP include: M.G. received funding from THL, Finnish Institute for Health and Welfare to support data collection. K.D. received funding from EDCTP RIA2019 and HDRUK (grant #2020.106) to support data collection. R.B. received funding from Alzheimer’s Disease Data Initiative and ICODA for the development of federated analysis. A.D.M. received funding from HDR UK who receives its funding from the UK Medical Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Government), Public Health Agency (Northern Ireland), British Heart Foundation (BHF) and the Wellcome Trust; and Administrative Data Research UK, which is funded by the Economic and Social Research Council (grant ES/S007393/1). N.A. received funding from the National Institutes of Health (R35GM138353). O.S received funding from NordForsk (grant #105545). The remaining authors declare no competing interests.
Figures











References
-
- Vogel, J. P. et al. The global epidemiology of preterm birth. Best. Pract. Res. Clin. Obstet. Gynaecol.52, 3–12 (2018). - PubMed
-
- Blencowe, H. et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. Lancet Glob. Health4, e98–e108 (2016). - PubMed
