

Evaluating elimination thresholds and stopping criteria for interventions against the vector-borne macroparasitic disease, lymphatic filariasis, using mathematical modelling
- PMID: 36849730
- PMCID: PMC9971242
- DOI: 10.1038/s42003-022-04391-9
Evaluating elimination thresholds and stopping criteria for interventions against the vector-borne macroparasitic disease, lymphatic filariasis, using mathematical modelling
Abstract
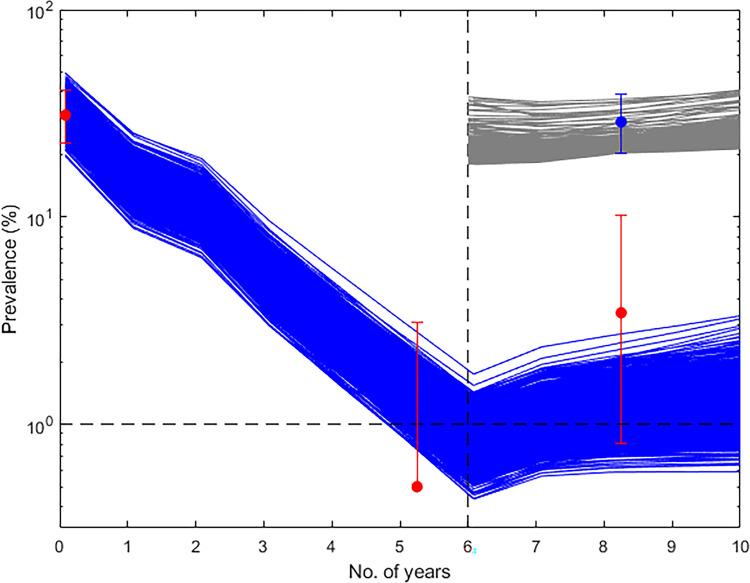
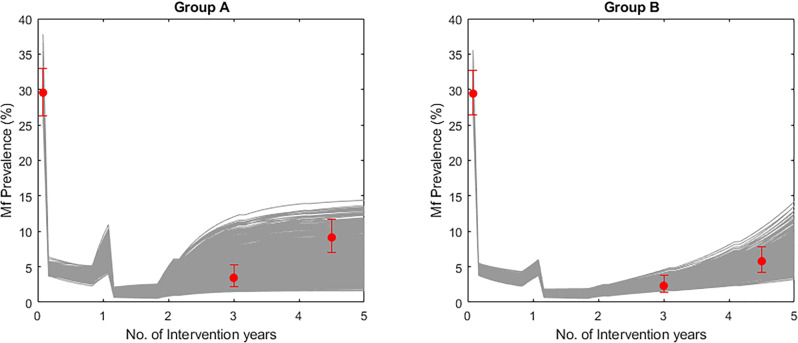
We leveraged the ability of EPIFIL transmission models fit to field data to evaluate the use of the WHO Transmission Assessment Survey (TAS) for supporting Lymphatic Filariasis (LF) intervention stopping decisions. Our results indicate that understanding the underlying parasite extinction dynamics, particularly the protracted transient dynamics involved in shifts to the extinct state, is crucial for understanding the impacts of using TAS for determining the achievement of LF elimination. These findings warn that employing stopping criteria set for operational purposes, as employed in the TAS strategy, without a full consideration of the dynamics of extinction could seriously undermine the goal of achieving global LF elimination.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Continental-scale, data-driven predictive assessment of eliminating the vector-borne disease, lymphatic filariasis, in sub-Saharan Africa by 2020.BMC Med. 2017 Sep 27;15(1):176. doi: 10.1186/s12916-017-0933-2. BMC Med. 2017. PMID: 28950862 Free PMC article.
-
Geographic and ecologic heterogeneity in elimination thresholds for the major vector-borne helminthic disease, lymphatic filariasis.BMC Biol. 2010 Mar 17;8:22. doi: 10.1186/1741-7007-8-22. BMC Biol. 2010. PMID: 20236528 Free PMC article.
-
Bayesian calibration of simulation models for supporting management of the elimination of the macroparasitic disease, Lymphatic Filariasis.Parasit Vectors. 2015 Oct 22;8:522. doi: 10.1186/s13071-015-1132-7. Parasit Vectors. 2015. PMID: 26490350 Free PMC article.
-
Elimination of lymphatic filariasis as a public health problem from the Arab Republic of Egypt.Acta Trop. 2019 Nov;199:105121. doi: 10.1016/j.actatropica.2019.105121. Epub 2019 Aug 7. Acta Trop. 2019. PMID: 31400299 Review.
-
Modelling lymphatic filariasis transmission and control: modelling frameworks, lessons learned and future directions.Adv Parasitol. 2015 Mar;87:249-91. doi: 10.1016/bs.apar.2014.12.005. Epub 2015 Feb 13. Adv Parasitol. 2015. PMID: 25765197 Review.
Cited by
-
Reducing the Antigen Prevalence Target Threshold for Stopping and Restarting Mass Drug Administration for Lymphatic Filariasis Elimination: A Model-Based Cost-effectiveness Simulation in Tanzania, India and Haiti.Clin Infect Dis. 2024 Apr 25;78(Suppl 2):S160-S168. doi: 10.1093/cid/ciae108. Clin Infect Dis. 2024. PMID: 38662697 Free PMC article.
-
Integrated survey of helminthic neglected tropical diseases and comparison of two mosquito sampling methods for lymphatic filariasis molecular xenomonitoring in the River Galana area, Kilifi County, coastal Kenya.PLoS One. 2022 Dec 9;17(12):e0278655. doi: 10.1371/journal.pone.0278655. eCollection 2022. PLoS One. 2022. PMID: 36490233 Free PMC article.
References
-
- Fact Sheet: Lymphatic Filariasis [Internet]. Geneva, Switzerland: World Health Organization, http://www.who.int/mediacentre/factsheets/fs102/en/ (2012).
-
- World Health Organization. in Global Programme to Eliminate Lymphatic Filariasis: Monitoring and Epidemiological Assessment of Mass Drug Administration: A Manual for National Elimination Programs. 22–33 (WHO, 2011).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
