

Ethnic disparities in COVID-19 outcomes: a multinational cohort study of 20 million individuals from England and Canada
- PMID: 36849983
- PMCID: PMC9969387
- DOI: 10.1186/s12889-023-15223-8
Ethnic disparities in COVID-19 outcomes: a multinational cohort study of 20 million individuals from England and Canada
Abstract
Background: Heterogeneous studies have demonstrated ethnic inequalities in the risk of SARS-CoV-2 infection and adverse COVID-19 outcomes. This study evaluates the association between ethnicity and COVID-19 outcomes in two large population-based cohorts from England and Canada and investigates potential explanatory factors for ethnic patterning of severe outcomes.
Methods: We identified adults aged 18 to 99 years in the QResearch primary care (England) and Ontario (Canada) healthcare administrative population-based datasets (start of follow-up: 24th and 25th Jan 2020 in England and Canada, respectively; end of follow-up: 31st Oct and 30th Sept 2020, respectively). We harmonised the definitions and the design of two cohorts to investigate associations between ethnicity and COVID-19-related death, hospitalisation, and intensive care (ICU) admission, adjusted for confounders, and combined the estimates obtained from survival analyses. We calculated the 'percentage of excess risk mediated' by these risk factors in the QResearch cohort.
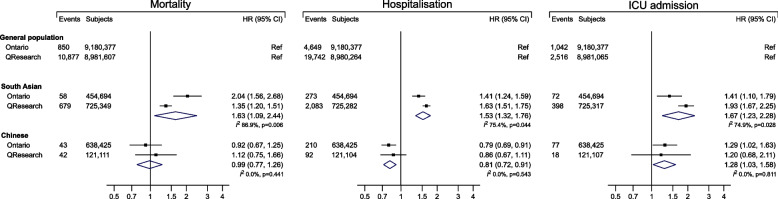
Results: There were 9.83 million adults in the QResearch cohort (11,597 deaths; 21,917 hospitalisations; 2932 ICU admissions) and 10.27 million adults in the Ontario cohort (951 deaths; 5132 hospitalisations; 1191 ICU admissions). Compared to the general population, pooled random-effects estimates showed that South Asian ethnicity was associated with an increased risk of COVID-19 death (hazard ratio: 1.63, 95% CI: 1.09-2.44), hospitalisation (1.53; 1.32-1.76), and ICU admission (1.67; 1.23-2.28). Associations with ethnic groups were consistent across levels of deprivation. In QResearch, sociodemographic, lifestyle, and clinical factors accounted for 42.9% (South Asian) and 39.4% (Black) of the excess risk of COVID-19 death.
Conclusion: International population-level analyses demonstrate clear ethnic inequalities in COVID-19 risks. Policymakers should be cognisant of the increased risks in some ethnic populations and design equitable health policy as the pandemic continues.
Keywords: COVID-19; Canada; Ethnicity; Hospitalisation; Inequalities; Mortality; UK.
© 2023. The Author(s).
Conflict of interest statement
KK is a Member of the Scientific Advisory Group for Emergencies (SAGE), Member of Independent SAGE, Director of the University of Leicester Centre for Black Minority Health and Trustee of the South Asian Health Foundation. JHC is a member of several SAGE committees and chair of the risk stratification subgroup of the NERVTAG. She is unpaid director of QResearch and founder and former medical director of ClinRisk Ltd. (outside the submitted work). PST reports past consultation with AstraZeneca and Duke-NUS outside the submitted work. All other authors have no competing interests to declare.
JHC is an unpaid director of QResearch, a not-for-profit organisation which is a partnership between the University of Oxford and EMIS Health who supply the QResearch database used for this work, and is a founder and shareholder of ClinRisk Ltd. and was its medical director until 31 May 2019; ClinRisk produces open and closed source software to implement clinical risk algorithms (outside this work) into clinical computer systems.
Figures
References
-
- Coronavirus cases: Reported Cases and Deaths by Country, Territory, or Conveyance. https://www.worldometers.info/coronavirus/ (Accessed 3 Aug 2021).
-
- Mathur R, Rentsch CT, Morton CE, et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: an observational cohort study using the OpenSAFELY platform. Lancet. 2021;397(10286):1711–1724. doi: 10.1016/S0140-6736(21)00634-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
