

TGF-β is elevated in hyperuricemic individuals and mediates urate-induced hyperinflammatory phenotype in human mononuclear cells
- PMID: 36850003
- PMCID: PMC9969669
- DOI: 10.1186/s13075-023-03001-1
TGF-β is elevated in hyperuricemic individuals and mediates urate-induced hyperinflammatory phenotype in human mononuclear cells
Abstract
Background: Soluble urate leads to a pro-inflammatory phenotype in human monocytes characterized by increased production of IL-1β and downregulation of IL-1 receptor antagonist, the mechanism of which remains to be fully elucidated. Previous transcriptomic data identified differential expression of genes in the transforming growth factor (TGF)-β pathway in monocytes exposed to urate in vitro. In this study, we explore the role of TGF-β in urate-induced hyperinflammation in peripheral blood mononuclear cells (PBMCs).
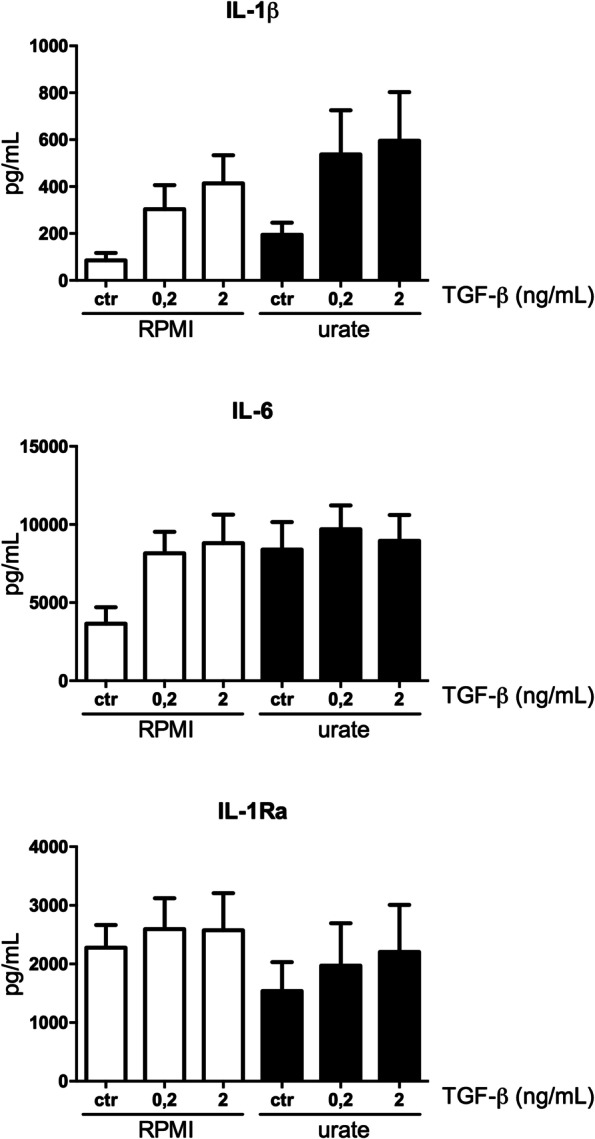
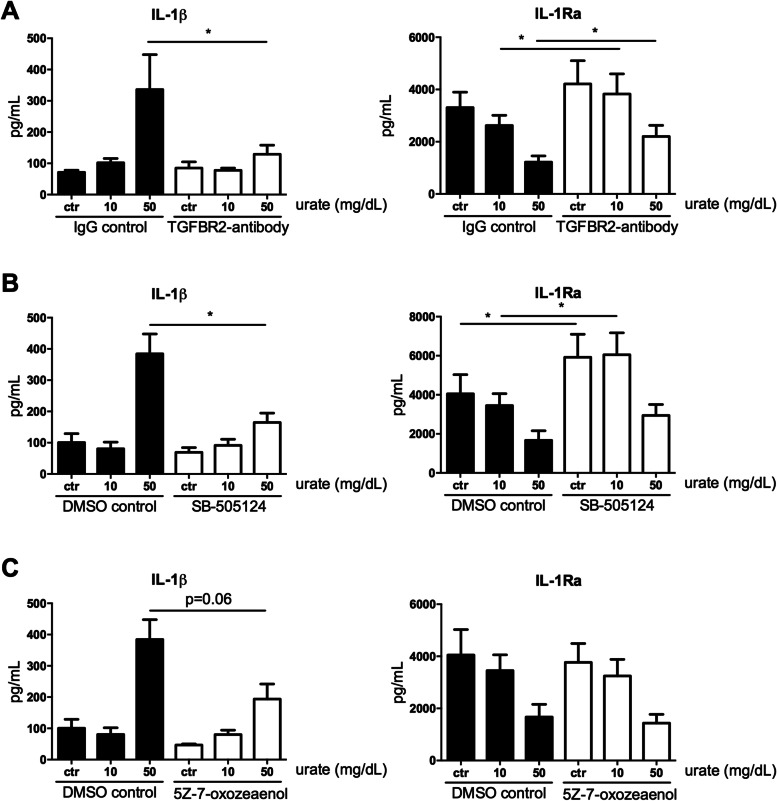
Methods: TGF-β mRNA in unstimulated PBMCs and protein levels in plasma were measured in individuals with normouricemia, hyperuricemia and gout. For in vitro validation, PBMCs of healthy volunteers were isolated and treated with a dose ranging concentration of urate for assessment of mRNA and pSMAD2. Urate and TGF-β priming experiments were performed with three inhibitors of TGF-β signalling: SB-505124, 5Z-7-oxozeaenol and a blocking antibody against TGF-β receptor II.
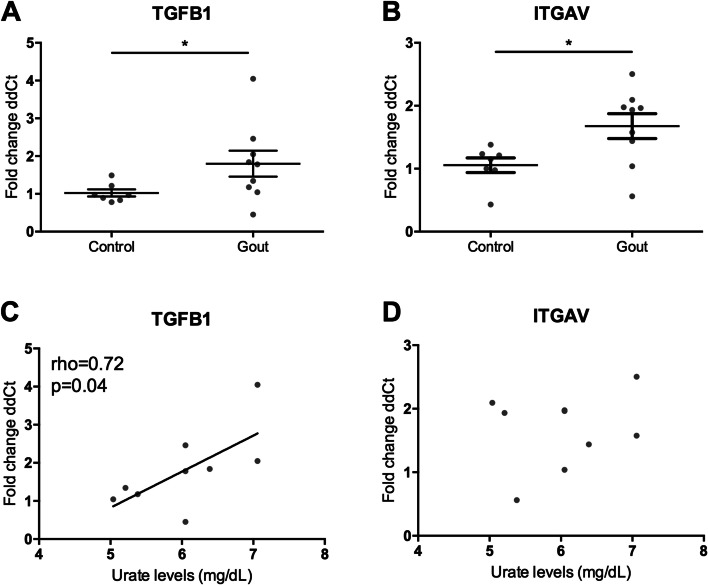
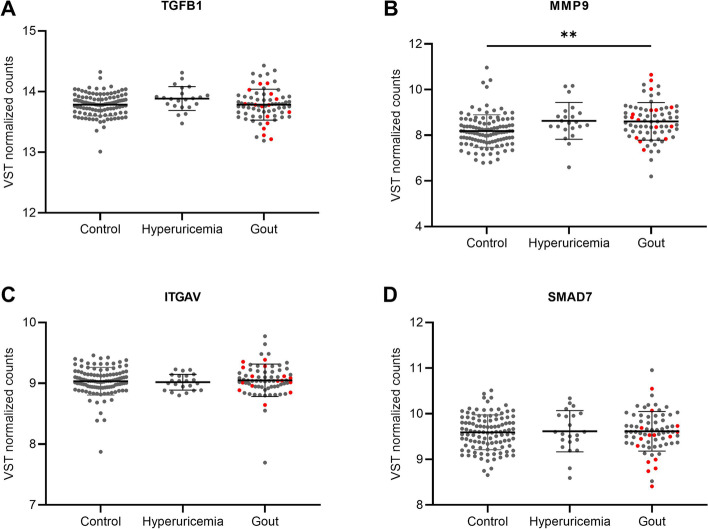
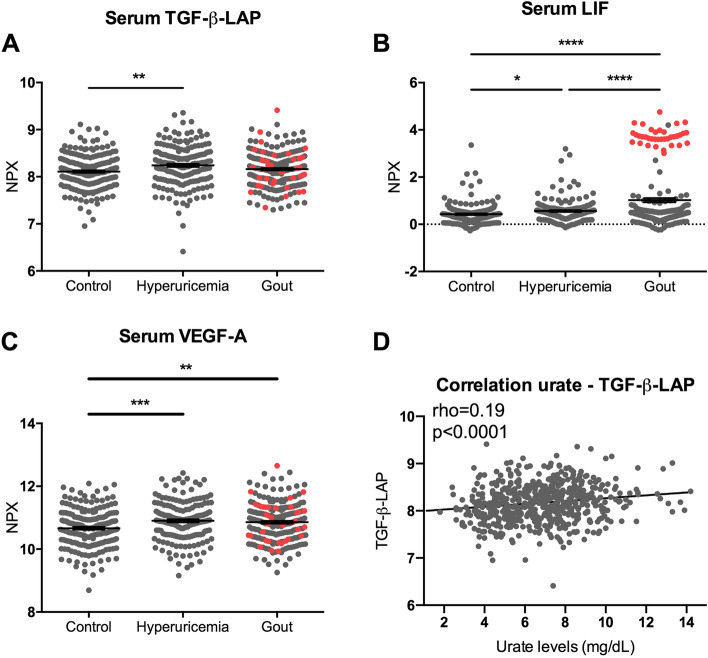
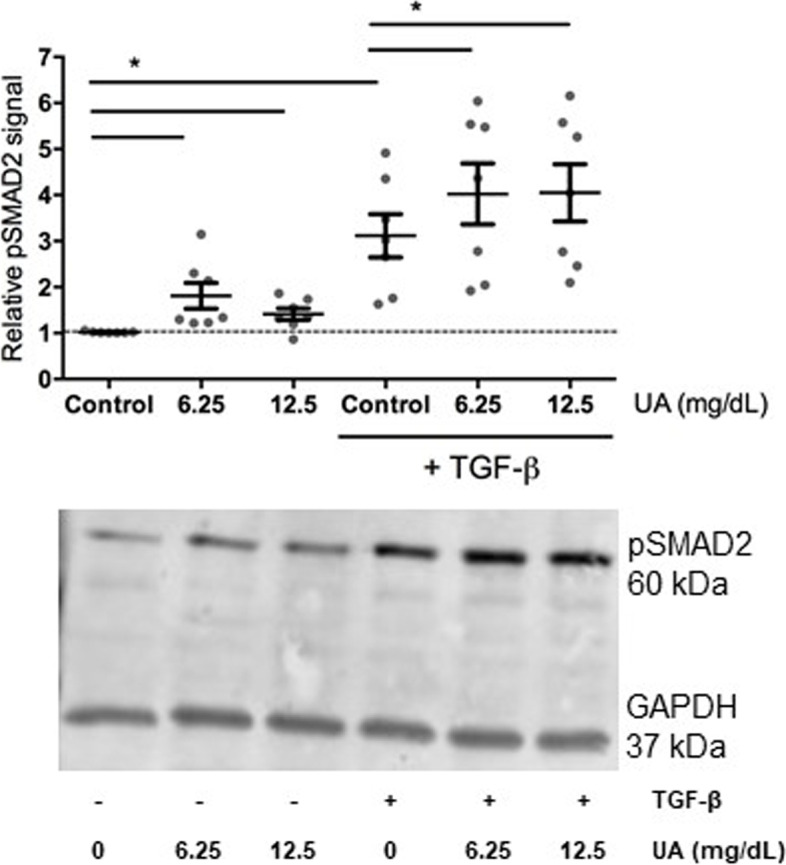
Results: TGF-β mRNA levels were elevated in gout patients compared to healthy controls. TGF-β-LAP levels in serum were significantly higher in individuals with hyperuricemia compared to controls. In both cases, TGF-β correlated positively to serum urate levels. In vitro, urate exposure of PBMCs did not directly induce TGF-β but did enhance SMAD2 phosphorylation. The urate-induced pro-inflammatory phenotype of monocytes was partly reversed by blocking TGF-β.
Conclusions: TGF-β is elevated in individuals with hyperuricemia and correlated to serum urate concentrations. In addition, the urate-induced pro-inflammatory phenotype in human monocytes is mediated by TGF-β signalling. Future studies are warranted to explore the intracellular pathways involved and to assess the clinical significance of urate-TGF-β relation.
Keywords: Hyperuricemia; Inflammation; Mononuclear leukocytes; TGF-β.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Joosten LA, Netea MG, Mylona E, Koenders MI, Malireddi RK, Oosting M, et al. Engagement of fatty acids with Toll-like receptor 2 drives interleukin-1beta production via the ASC/caspase 1 pathway in monosodium urate monohydrate crystal-induced gouty arthritis. Arthritis Rheum. 2010;62(11):3237–3248. doi: 10.1002/art.27667. - DOI - PMC - PubMed
-
- So A, Dumusc A, Nasi S. The role of IL-1 in gout: from bench to bedside. Rheumatology (Oxford) 2018;57(suppl_1):i12–ii9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
