

Characteristics and outcomes of an international cohort of 600 000 hospitalized patients with COVID-19
- PMID: 36850054
- PMCID: PMC10114094
- DOI: 10.1093/ije/dyad012
Characteristics and outcomes of an international cohort of 600 000 hospitalized patients with COVID-19
Abstract
Background: We describe demographic features, treatments and clinical outcomes in the International Severe Acute Respiratory and emerging Infection Consortium (ISARIC) COVID-19 cohort, one of the world's largest international, standardized data sets concerning hospitalized patients.
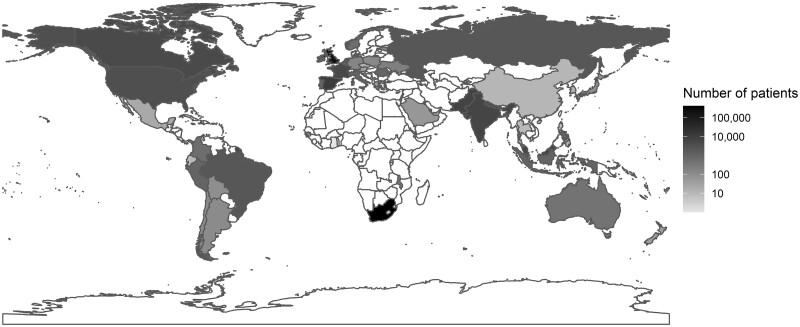
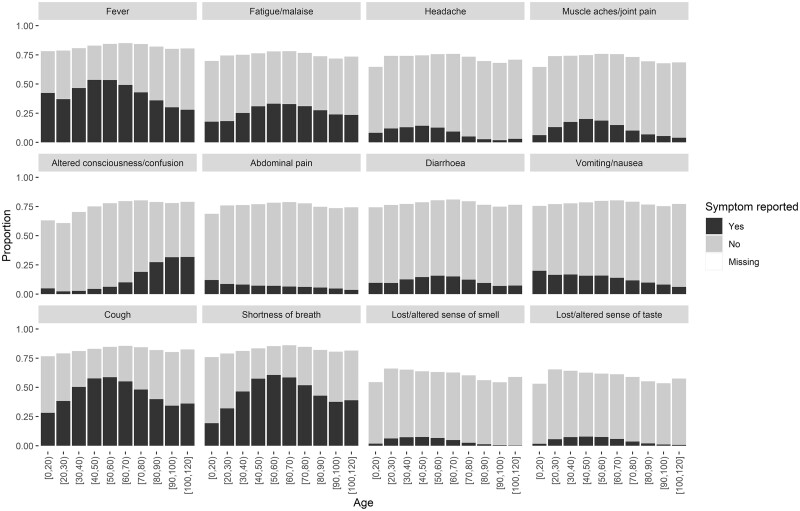
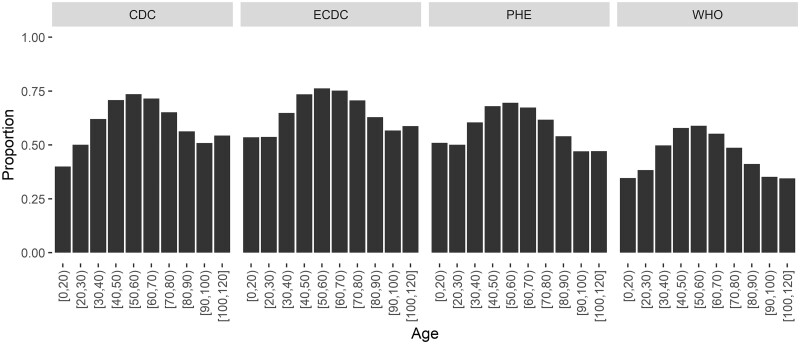
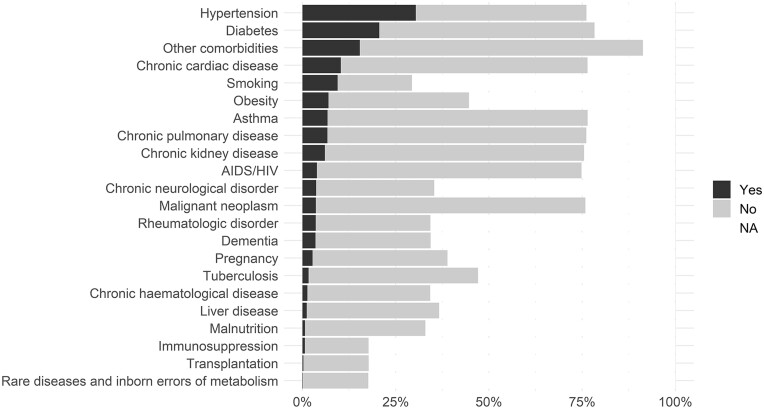
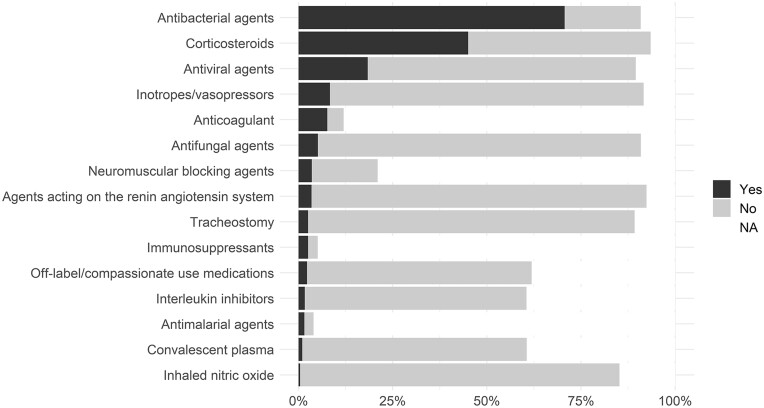
Methods: The data set analysed includes COVID-19 patients hospitalized between January 2020 and January 2022 in 52 countries. We investigated how symptoms on admission, co-morbidities, risk factors and treatments varied by age, sex and other characteristics. We used Cox regression models to investigate associations between demographics, symptoms, co-morbidities and other factors with risk of death, admission to an intensive care unit (ICU) and invasive mechanical ventilation (IMV).
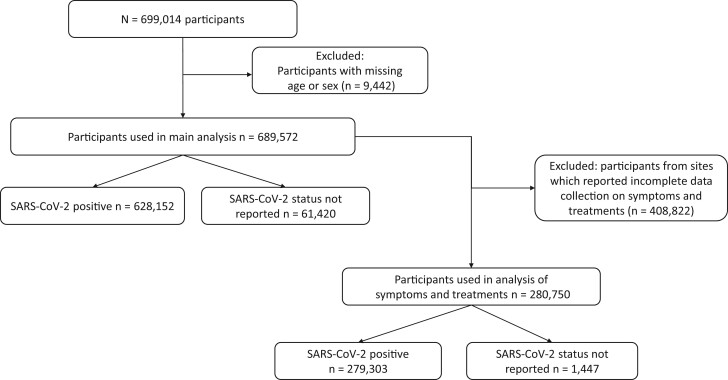
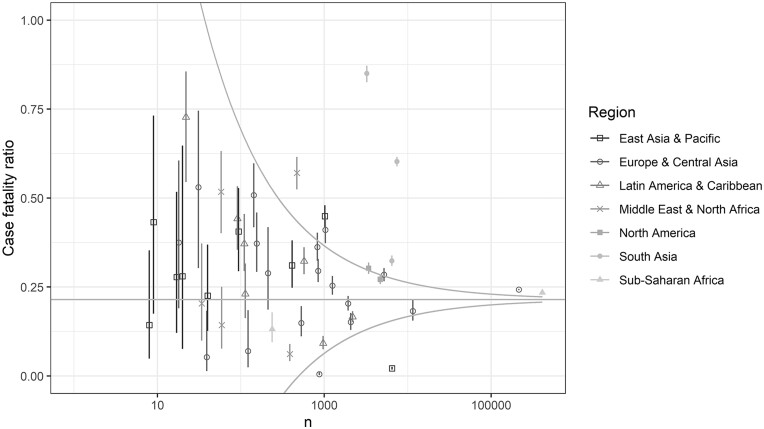
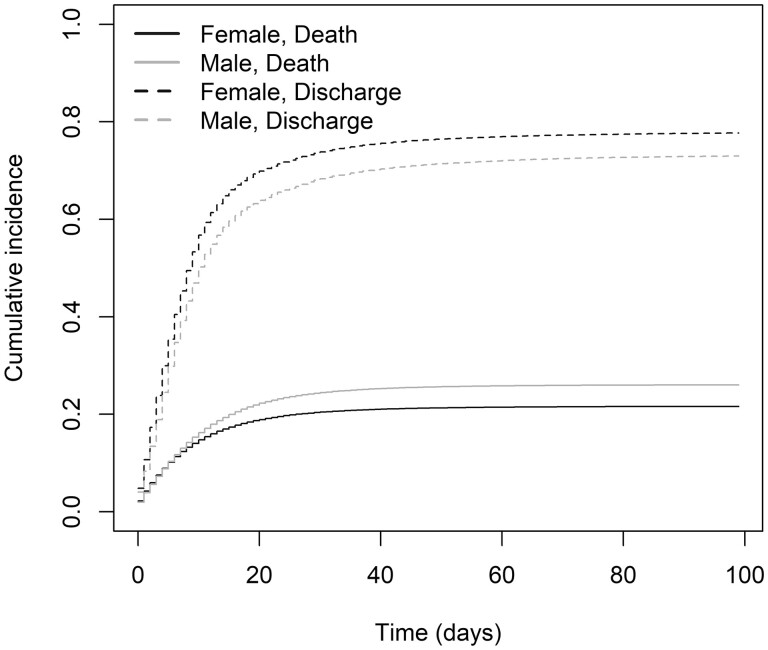
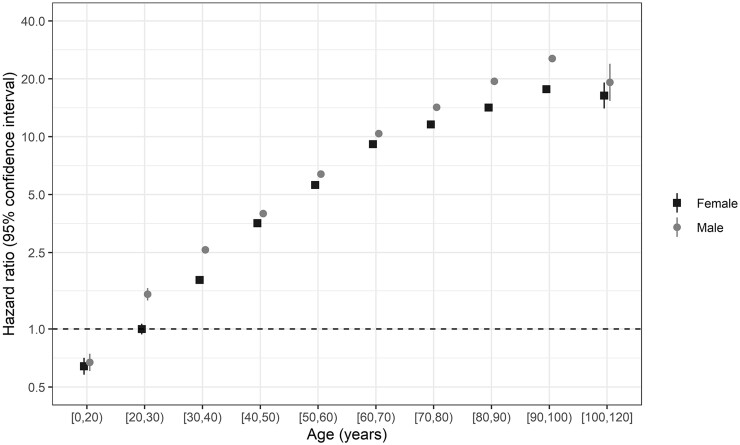
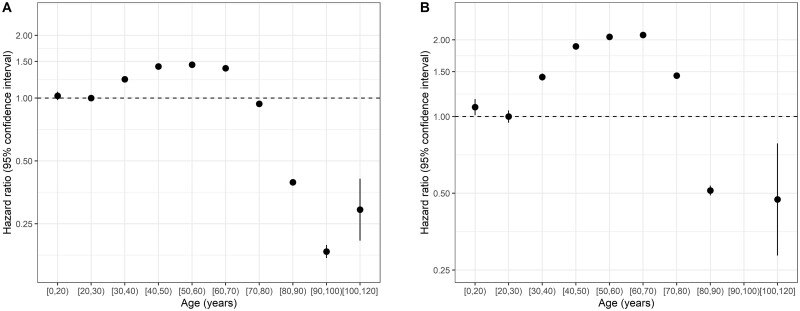
Results: Data were available for 689 572 patients with laboratory-confirmed (91.1%) or clinically diagnosed (8.9%) SARS-CoV-2 infection from 52 countries. Age [adjusted hazard ratio per 10 years 1.49 (95% CI 1.48, 1.49)] and male sex [1.23 (1.21, 1.24)] were associated with a higher risk of death. Rates of admission to an ICU and use of IMV increased with age up to age 60 years then dropped. Symptoms, co-morbidities and treatments varied by age and had varied associations with clinical outcomes. The case-fatality ratio varied by country partly due to differences in the clinical characteristics of recruited patients and was on average 21.5%.
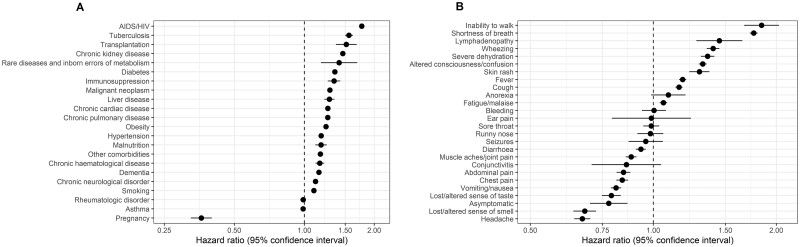
Conclusions: Age was the strongest determinant of risk of death, with a ∼30-fold difference between the oldest and youngest groups; each of the co-morbidities included was associated with up to an almost 2-fold increase in risk. Smoking and obesity were also associated with a higher risk of death. The size of our international database and the standardized data collection method make this study a comprehensive international description of COVID-19 clinical features. Our findings may inform strategies that involve prioritization of patients hospitalized with COVID-19 who have a higher risk of death.
Keywords: COVID-19; SARS-CoV-2; co-morbidities; cohort study; risk of death; symptoms; treatments.
© The Author(s) 2023. Published by Oxford University Press on behalf of the International Epidemiological Association.
Conflict of interest statement
Donnelly, C.A. declares research funding from the UK Medical Research Council and the UK National Institute for Health Research. Ho, A. declares grant funding from Medical Research Council UK, Scottish Funding Council—Grand Challenges Research Fund, and the Wellcome Trust, outside this submitted work. Martin-Loeches I. declared lectures for Gilead, Thermofisher, Pfizer, MSD; advisory board participation for Fresenius Kabi, Advanz Pharma, Gilead, Accelerate, Merck; and consulting fees for Gilead outside of the submitted work. Mentré F, declares consulting fees from IPSEN, Servier and Da Volterra, and reports research grants to her group from Sanofi, Roche, Servier and Da Voleterra, all outside the submitted work. Nichol, A. declares a grant from the Health Research Board of Ireland to support data collection in Ireland (CTN-2014–012), an unrestricted grant from BAXTER for the TAME trial kidney substudy and consultancy fees paid to his institution from AM-PHARMA. Semple, M.G. reports grants from DHSC National Institute of Health Research UK, from the Medical Research Council UK and from the Health Protection Research Unit in Emerging & Zoonotic Infections, University of Liverpool, supporting the conduct of the study; other interest in Integrum Scientific LLC, Greensboro, NC, USA, outside the submitted work. Streinu-Cercel, Anca has been an investigator in COVID-19 clinical trials by Algernon Pharmaceuticals, Atea Pharmaceuticals, Regeneron Pharmaceuticals, Diffusion Pharmaceuticals, Celltrion, Inc. and Atriva Therapeutics, outside the scope of the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- CO-CIN-01/DH_/Department of Health/United Kingdom
- U01 HL123009/HL/NHLBI NIH HHS/United States
- IS-BRC-1215–20013/DH_/Department of Health/United Kingdom
- MR/R015600/1/MRC_/Medical Research Council/United Kingdom
- MR/V001329/1/MRC_/Medical Research Council/United Kingdom
- 200907/DH_/Department of Health/United Kingdom
- MC_PC_19026/MRC_/Medical Research Council/United Kingdom
- 205228/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MR/S032304/1/MRC_/Medical Research Council/United Kingdom
- NIHR201385/DH_/Department of Health/United Kingdom
- 200927/DH_/Department of Health/United Kingdom
- OPP1209135/GATES/Gates Foundation/United States
- MR/V030884/1/MRC_/Medical Research Council/United Kingdom
- MR/V001671/1/MRC_/Medical Research Council/United Kingdom
- 215091/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- 220757/Z/20/Z/WT_/Wellcome Trust/United Kingdom
