

The Impact of Corticosteroids on the Outcome of Fungal Disease: a Systematic Review and Meta-analysis
- PMID: 36852004
- PMCID: PMC9947451
- DOI: 10.1007/s12281-023-00456-2
The Impact of Corticosteroids on the Outcome of Fungal Disease: a Systematic Review and Meta-analysis
Abstract
Purpose of review: Corticosteroids have a complex relationship with fungal disease - risk for many, benefit for others. This systematic review aims to address the effect of corticosteroids on mortality and visual outcome in different fungal diseases.
Recent findings: Corticosteroids are a risk factor of aspergillosis for patients who have COVID-19, and they also led to a worse outcome. Similarity, corticosteroids are a risk factor for candidemia and mucormycosis. Some researchers reported that using topical corticosteroid in keratitis was associated with worse visual outcome if fungal keratitis. Some studies showed that corticosteroids are linked to a negative outcome for non-HIV patients with Pneumocystis jirovecii pneumonia (PCP), in contrast to those with HIV and PCP.
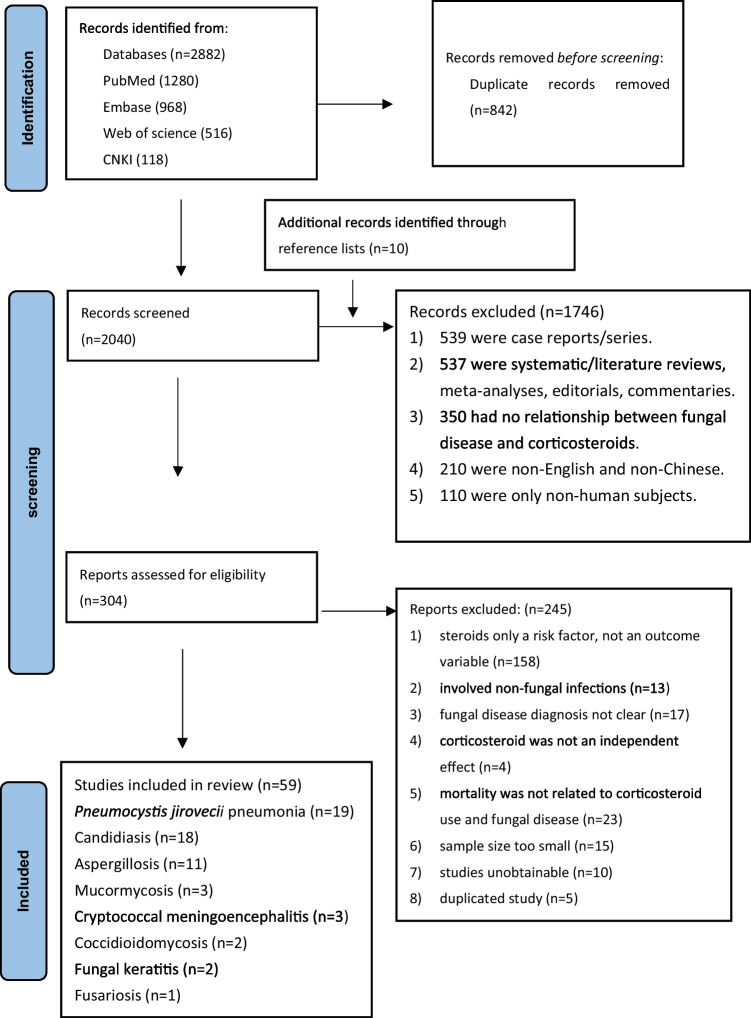
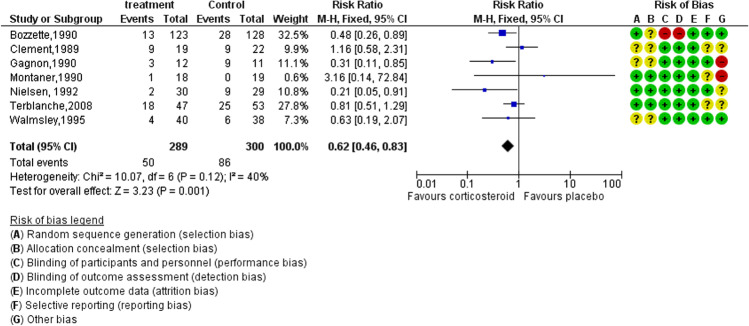
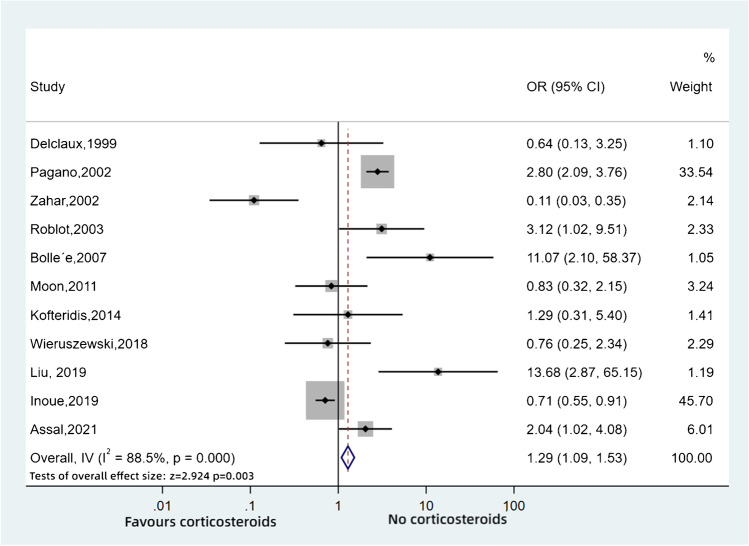
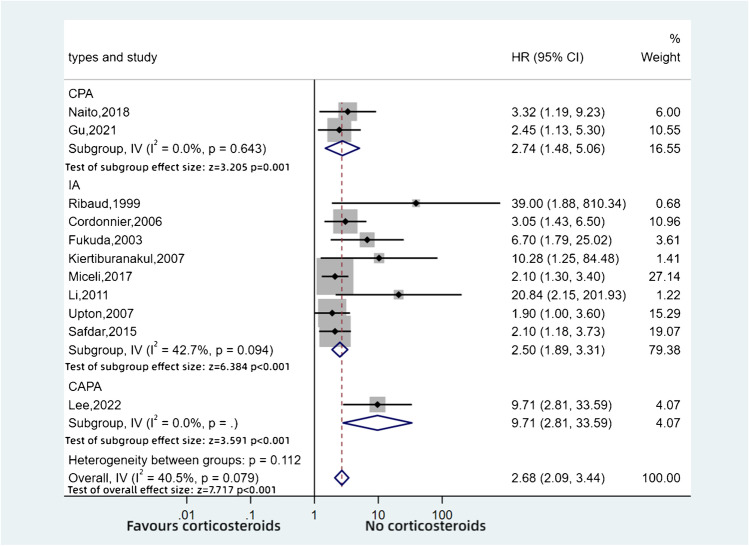
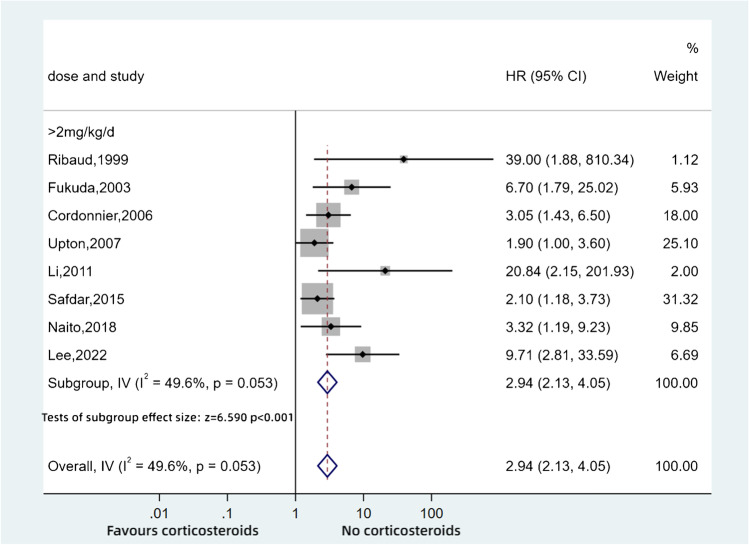
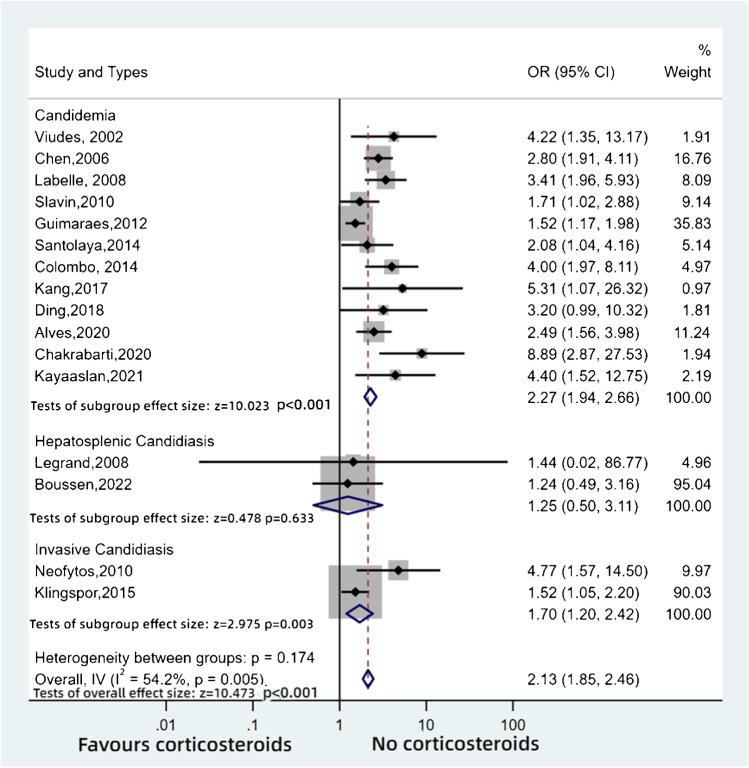
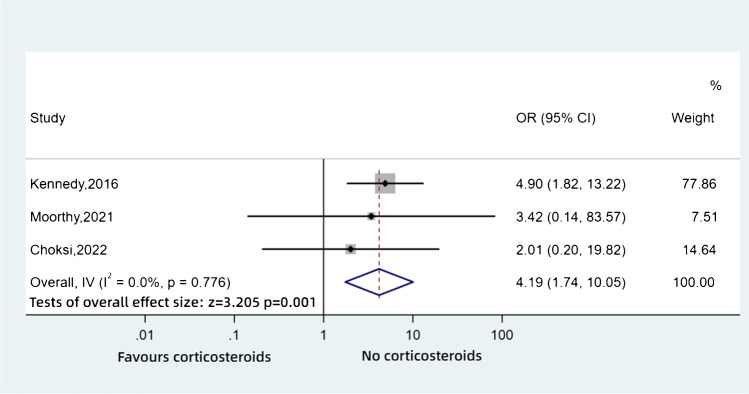
Summary: In 59 references, we found that corticosteroid therapy showed a worse clinical outcome in invasive aspergillosis (IA) (HR: 2.50, 95%CI: 1.89-3.31, p < 0.001) and chronic pulmonary aspergillosis (CPA) (HR: 2.74, 95%CI: 1.48-5.06, p = 0.001), PCP without HIV infection (OR: 1.29, 95%CI: 1.09-1.53, p = 0.003), invasive candidiasis and candidaemia (OR: 2.13, 95%CI: 1.85-2.46, p < 0.001), mucormycosis (OR: 4.19, 95%CI: 1.74-10.05, p = 0.001) and early in the course of fungal keratitis (OR: 2.99, 95%CI: 1.14-7.84, p = 0.026). There was equivocal outcome in cryptococcal meningoencephalitis in AIDS and primary coccidioidomycosis, while corticosteroid therapy showed a better outcome in PCP in HIV-infected patients (RR: 0.62, 95%CI: 0.46-0.83, p=0.001) and fungal keratitis patients after keratoplasty surgery (OR: 0.01, 95%CI: 0.00-0.41, p = 0.041) and probably in cryptococcal meningoencephalitis in non-immunocompromised patients. A sub-analysis in invasive aspergillosis and CPA showed that use of more than 2 mg/kg/day of prednisolone equivalents per day is a significant factor in increasing mortality (HR: 2.94, 95%CI: 2.13-4.05, p < 0.001). Corticosteroid therapy during invasive fungal disease was usually associated with a slightly or greatly increased mortality or worse visual outcome (in fungal keratitis), with two disease exceptions. Avoiding the addition of corticosteroids, or minimising dose and duration in those who require them, is likely to improve the outcome of most life- and vision-threatening fungal diseases. This review provides a cornerstone for further research in exploring the accuracy of suitable dose and duration of corticosteroids treatment in fungal diseases.
Supplementary information: The online version contains supplementary material available at 10.1007/s12281-023-00456-2.
Keywords: Blindness; Fungal disease; Hydrocortisone; Methylprednisolone; Prednisolone.
© The Author(s) 2023.
Conflict of interest statement
Conflict of InterestThe authors declare no competing interests.
Figures
Similar articles
-
Diagnostic performance of the (1-3)-β-D-glucan assay in patients with Pneumocystis jirovecii compared with those with candidiasis, aspergillosis, mucormycosis, and tuberculosis, and healthy volunteers.PLoS One. 2017 Nov 30;12(11):e0188860. doi: 10.1371/journal.pone.0188860. eCollection 2017. PLoS One. 2017. PMID: 29190812 Free PMC article.
-
Burden of serious fungal infections in Tanzania.Mycoses. 2015 Oct;58 Suppl 5:70-9. doi: 10.1111/myc.12390. Mycoses. 2015. PMID: 26449510
-
Estimated Burden of Serious Fungal Infections in Ghana.J Fungi (Basel). 2019 May 11;5(2):38. doi: 10.3390/jof5020038. J Fungi (Basel). 2019. PMID: 31083531 Free PMC article.
-
Common invasive fungal diseases: an overview of invasive candidiasis, aspergillosis, cryptococcosis, and Pneumocystis pneumonia.Swiss Med Wkly. 2016 Feb 22;146:w14281. doi: 10.4414/smw.2016.14281. eCollection 2016. Swiss Med Wkly. 2016. PMID: 26901377 Review.
-
The Burden of Fungal Infections in Ethiopia.J Fungi (Basel). 2019 Nov 22;5(4):109. doi: 10.3390/jof5040109. J Fungi (Basel). 2019. PMID: 31771096 Free PMC article. Review.
Cited by
-
Candidemia chronicles: Retrospective analysis of candidemia epidemiology, species distribution, and antifungal susceptibility patterns in Bahrain.World J Virol. 2024 Dec 25;13(4):98839. doi: 10.5501/wjv.v13.i4.98839. World J Virol. 2024. PMID: 39722764 Free PMC article.
-
COVID-19 associated with cryptococcosis: a scoping review.Ther Adv Infect Dis. 2024 Feb 14;11:20499361241232851. doi: 10.1177/20499361241232851. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 38361915 Free PMC article.
-
Unveiling ferroptosis genes and inhibitors in diabetic retinopathy through single-cell analysis and docking simulations.Biochem Biophys Rep. 2025 Jan 31;41:101932. doi: 10.1016/j.bbrep.2025.101932. eCollection 2025 Mar. Biochem Biophys Rep. 2025. PMID: 39968183 Free PMC article.
-
Current Analytical Methods and Challenges for the Clinical Diagnosis of Invasive Pulmonary Aspergillosis Infection.J Fungi (Basel). 2024 Nov 28;10(12):829. doi: 10.3390/jof10120829. J Fungi (Basel). 2024. PMID: 39728325 Free PMC article. Review.
-
In vitro and preclinical evaluation of the antifungal activity of 6-methoxy-1 H-indole-2-carboxylic acid produced by Bacillus toyonensis strain OQ071612 formulated as nanosponge hydrogel.Microb Cell Fact. 2025 Apr 1;24(1):77. doi: 10.1186/s12934-025-02688-y. Microb Cell Fact. 2025. PMID: 40169999 Free PMC article.
References
-
- Akan H, Antia VP, Kouba M, Sinko J, Tănase AD, Vrhovac R, et al. Preventing invasive fungal disease in patients with haematological malignancies and the recipients of haematopoietic stem cell transplantation: practical aspects. J Antimicrob Chemother. 2013;68(suppl_3):iii5–iii16. - PubMed
-
- Takeda K, Imamura Y, Takazono T, Yoshida M, Ide S, Hirano K, et al. The risk factors for developing of chronic pulmonary aspergillosis in nontuberculous mycobacteria patients and clinical characteristics and outcomes in chronic pulmonary aspergillosis patients coinfected with nontuberculous mycobacteria. Med Mycol. 2015;54(2):120–127. doi: 10.1093/mmy/myv093. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials