

Functional evaluation of intracranial atherosclerotic stenosis by pressure ratio measurements
- PMID: 36852079
- PMCID: PMC9958418
- DOI: 10.1016/j.heliyon.2023.e13527
Functional evaluation of intracranial atherosclerotic stenosis by pressure ratio measurements
Abstract
Background: Fractional flow reserve is widely used for the functional evaluation of coronary artery stenosis. Some studies have similarly used the translesional pressure ratio measurements for the functional evaluation of intracranial atherosclerotic stenosis. In this paper, we aimed to investigate the relationship between pressure ratio and cerebral tissue perfusion by MR perfusion imaging and provided a non-invasive method for evaluating the functional significance of intracranial atherosclerotic stenosis.
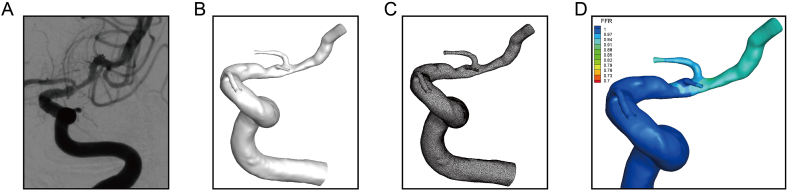
Methods: A total of 18 consecutive patients with intracranial atherosclerotic stenosis patients including 19 stenotic vessels were recruited. The pressure was measured using a pressure guidewire, the pressure ratio before and after the endovascular intervention was calculated and compared with the severity of diameter stenosis and perfusion-derived MR (the time to maximum tissure residue function (Tmax)). Moreover, the DSA-derived pressure ratio was computed using a novel computational fluid dynamics-based model, termed CFD-PR, and was compared with the actual pressure ratio to assess its diagnostic accuracy.
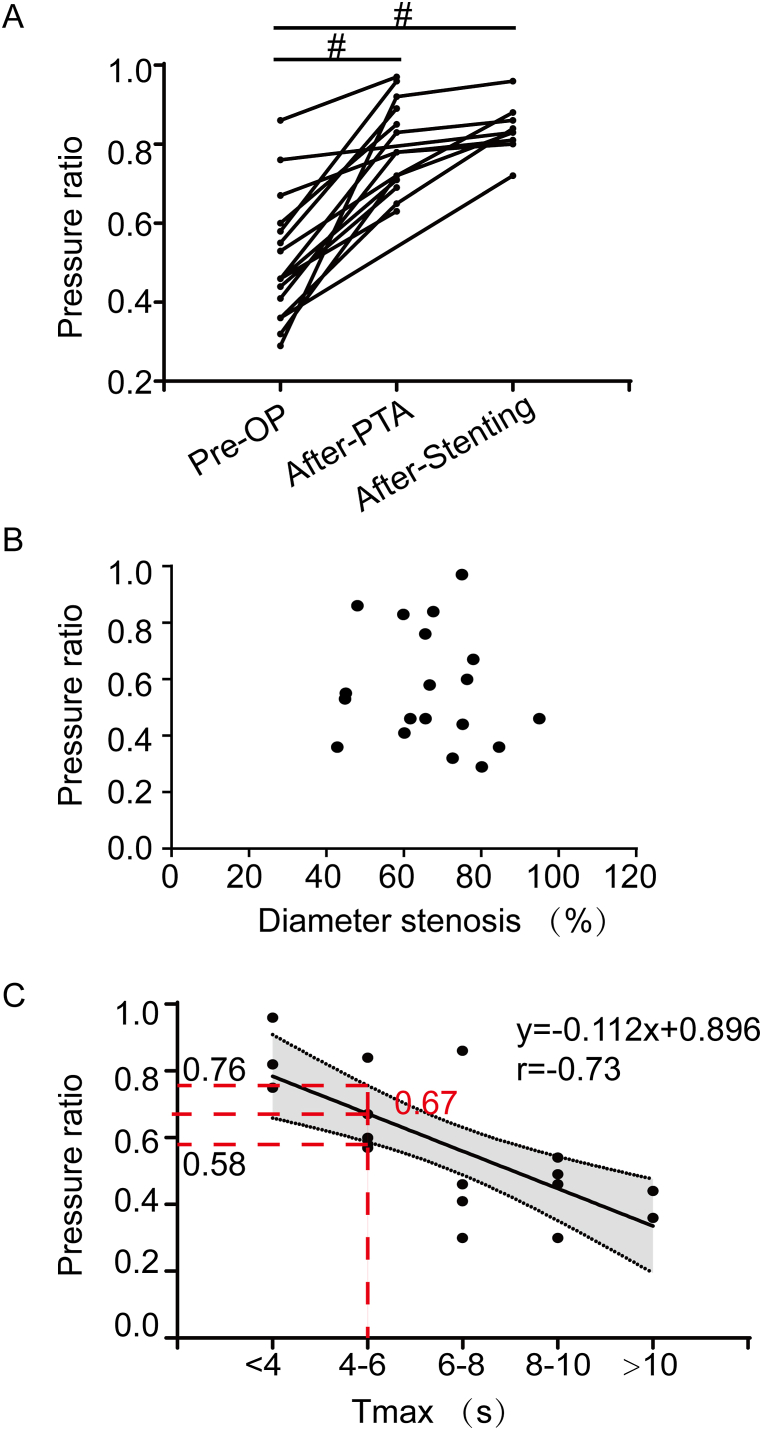
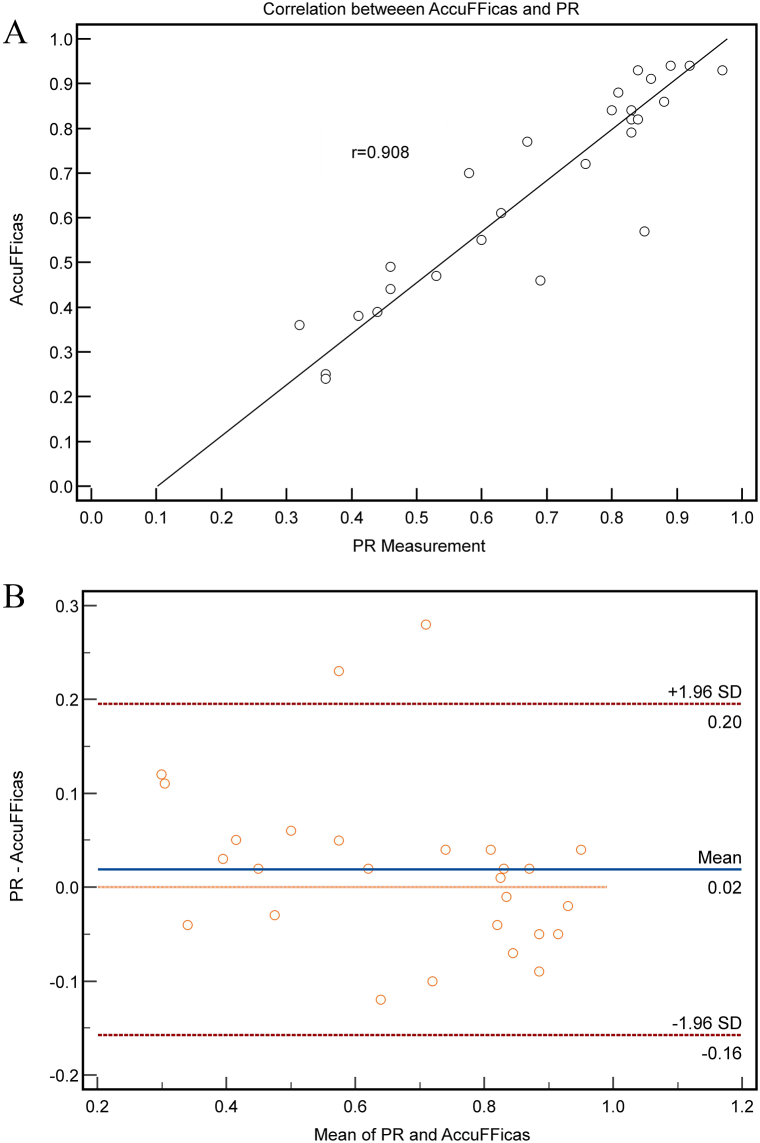
Results: The pressure ratio increased after percutaneous transluminal angioplasty or stenting, while the correlation between pressure ratio and diameter stenosis was not significant. The pressure ratio was negatively correlated with Tmax (r = -0.73, P < 0.01), and a 95% confidence interval for the cutoff value of pressure ratio = 0.67 (95% confidence interval: 0.58-0.76) was suggested. There was a good correlation (mean = 0.02, Spearman's correlation coefficient r = 0.908, P < 0.001) and agreement (limits of agreement: -0.157 to 0.196, P = 0.954) between CFD-PR and the actual pressure ratio.
Conclusions: This exploratory study indicates the pressure ratio may correlate with the perfusion status. The pressure ratio can be calculated through a non-invasive method using a computational fluid dynamics-based method.
Keywords: CFD, computational fluid dynamics; Cerebral ischemia; Computational fluid dynamics; DSA, digital subtraction angiography; FFR, fractional flow reserve; Fractional flow reserve; ICAS, intracranional flow reserve; Intracranial atherosclerotic stenosis; PCI, percutaneous coronary intervention; PR, pressure ratio; PTA, the percutaneous transluminal angioplasty; Pressure ratio; Tmax, the time to maximum tissue residue function.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Hemodynamic Impairments of Evaluating Symptomatic Intracranial Atherosclerotic Stenosis using Quantitative Flow Ratio on Digital Subtraction Angiography : A Comparison with Computed Tomography Perfusion, MRI and Fractional Flow Reserve.Clin Neuroradiol. 2024 Sep;34(3):613-624. doi: 10.1007/s00062-024-01395-2. Epub 2024 Mar 15. Clin Neuroradiol. 2024. PMID: 38489035
-
Noninvasive diagnosis of ischemia-causing coronary stenosis using CT angiography: diagnostic value of transluminal attenuation gradient and fractional flow reserve computed from coronary CT angiography compared to invasively measured fractional flow reserve.JACC Cardiovasc Imaging. 2012 Nov;5(11):1088-96. doi: 10.1016/j.jcmg.2012.09.002. JACC Cardiovasc Imaging. 2012. PMID: 23153908
-
Computed Tomography Coronary Angiography and Computational Fluid Dynamics Based Fractional Flow Reserve Before and After Percutaneous Coronary Intervention.Front Bioeng Biotechnol. 2021 Sep 7;9:739667. doi: 10.3389/fbioe.2021.739667. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34557479 Free PMC article.
-
Relationship Between Coronary Fractional Flow Reserve and Computational Fluid Dynamics Analysis in Moderate Stenosis of the Coronary Artery.Circ Rep. 2020 Sep 25;2(10):545-551. doi: 10.1253/circrep.CR-20-0078. Circ Rep. 2020. PMID: 33693179 Free PMC article. Review.
-
Non-invasive imaging software to assess the functional significance of coronary stenoses: a systematic review and economic evaluation.Health Technol Assess. 2021 Sep;25(56):1-230. doi: 10.3310/hta25560. Health Technol Assess. 2021. PMID: 34588097
Cited by
-
Hemodynamic Impairments of Evaluating Symptomatic Intracranial Atherosclerotic Stenosis using Quantitative Flow Ratio on Digital Subtraction Angiography : A Comparison with Computed Tomography Perfusion, MRI and Fractional Flow Reserve.Clin Neuroradiol. 2024 Sep;34(3):613-624. doi: 10.1007/s00062-024-01395-2. Epub 2024 Mar 15. Clin Neuroradiol. 2024. PMID: 38489035
-
Panvascular concept in the evaluation and treatment of intracranial atherosclerotic stenosis.Front Neurol. 2024 Dec 24;15:1460124. doi: 10.3389/fneur.2024.1460124. eCollection 2024. Front Neurol. 2024. PMID: 39777318 Free PMC article. Review.
-
Clinical implications of haemodynamics in symptomatic intracranial atherosclerotic stenosis by computational fluid dynamics modelling: a systematic review.Stroke Vasc Neurol. 2025 Feb 25;10(1):16-24. doi: 10.1136/svn-2024-003202. Stroke Vasc Neurol. 2025. PMID: 38806205 Free PMC article.
-
Differential sensitivities to blood pressure variations in internal carotid and intracranial arteries: a numerical approach to stroke prediction.Sci Rep. 2023 Dec 15;13(1):22319. doi: 10.1038/s41598-023-49591-3. Sci Rep. 2023. PMID: 38102319 Free PMC article.
-
Integrating hemodynamic analysis with traditional imaging in intracranial atherosclerotic stenosis: current status and future perspectives.Front Neurol. 2025 Jul 18;16:1589162. doi: 10.3389/fneur.2025.1589162. eCollection 2025. Front Neurol. 2025. PMID: 40757026 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
