

The inflammatory burden index is a superior systemic inflammation biomarker for the prognosis of non-small cell lung cancer
- PMID: 36852672
- PMCID: PMC10067487
- DOI: 10.1002/jcsm.13199
The inflammatory burden index is a superior systemic inflammation biomarker for the prognosis of non-small cell lung cancer
Abstract
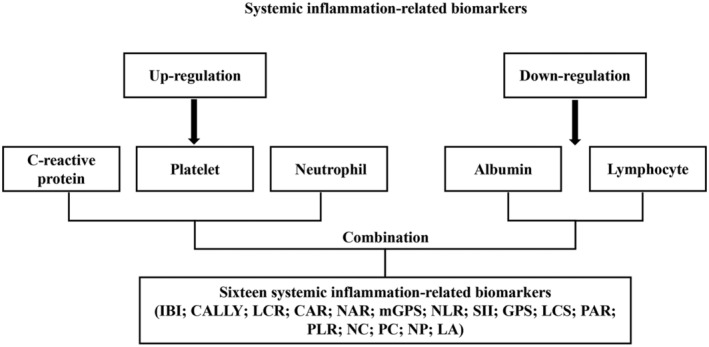
Background: Systemic inflammation, the most representative tumour-host interaction, plays a crucial role in disease progression and prognosis in patients with non-small cell lung cancer (NSCLC). Few studies have compared the performance of existing haematological systemic inflammation biomarkers in predicting the prognosis of NSCLC patients. The purpose of this study was to compare the prognostic value of existing systemic inflammation biomarkers and determine the optimal systemic inflammation biomarker in patients with NSCLC through a multicentre prospective study.
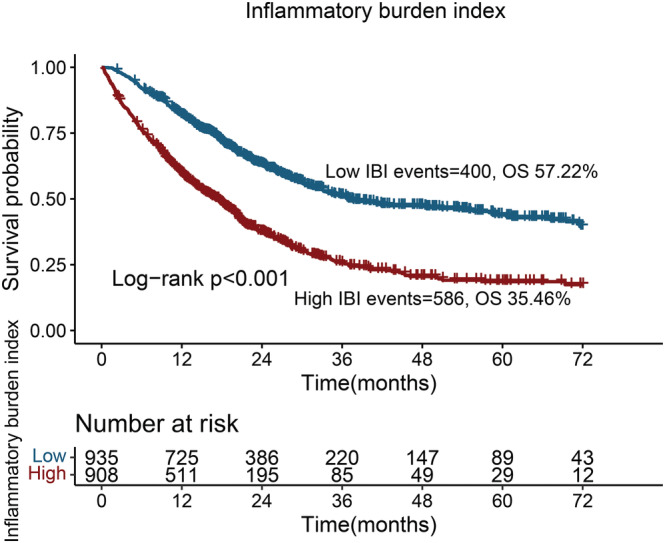
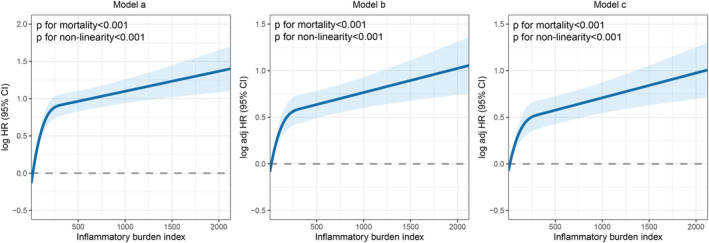
Methods: The predictive accuracy of systemic inflammation biomarkers for prognostic assessment in NSCLC was assessed using C-statistics. Inter-group differences in survival were assessed using the log-rank test and visualized using the Kaplan-Meier method. A restricted cubic spline (RCS) curve was used to explore the association between the biomarkers and survival. Independent prognostic biomarkers for overall survival were determined using multivariable Cox proportional hazards regression analysis. Logistic regression analysis was used to determine independent predictors of 90-day outcomes, length of hospitalization, hospitalization expenses and cachexia.
Results: The inflammatory burden index (IBI) had the highest C-statistic for predicting the prognosis of patients with NSCLC, reaching 0.640 (0.617, 0.663). Patients with a high IBI had significantly worse outcomes than those with a low IBI (35.46% vs. 57.22%; log-rank P < 0.001). The IBI was also able to differentiate the prognosis of patients with NSCLC with the same pathological stage. The RCS curve showed an inverted L-shaped dose-response relationship between the IBI and survival of patients with NSCLC. Multivariable Cox proportional hazards regression analysis showed that a high IBI was an independent risk factor for death of patients with NSCLC (hazard ratio = 1.229, 95% confidence interval [CI]: 1.131-1.335, P < 0.001). A high IBI was an independent predictor of 90-day outcomes (odds ratio [OR] = 1.789, 95% CI: 1.489-2.151, P < 0.001), prolonged hospital stays (OR = 1.560, 95% CI: 1.256-1.938, P < 0.001), high hospitalization expenses (OR = 1.476, 95% CI: 1.195-1.822, P < 0.001) and cachexia (OR = 1.741, 95%CI = 1.374-2.207, P < 0.001) in patients with NSCLC.
Conclusions: The IBI was independently associated with overall survival, 90-day outcomes, length of hospitalization, hospitalization expenses and cachexia in NSCLC patients. As an optimal systemic inflammation biomarker, the IBI has broad clinical application prospects in predicting the prognosis of patients with NSCLC.
Keywords: Biomarker; Cachexia; Expenses; Non-small cell lung cancer; Prognosis; Systemic inflammation.
© 2023 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Global Burden of Disease 2019 Cancer Collaboration , Kocarnik JM, Compton K, Dean FE, Fu W, Gaw BL, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability‐adjusted life years for 29 cancer groups from 2010 to 2019: a systematic analysis for the global burden of disease study 2019. JAMA Oncol 2022;8:420–444. - PMC - PubMed
-
- Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami‐Porta R, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol 2007;2:706–714. - PubMed
-
- Noma D, Inamura K, Matsuura Y, Hirata Y, Nakajima T, Yamazaki H, et al. Prognostic effect of lymphovascular invasion on TNM staging in stage I non‐small‐cell lung cancer. Clin Lung Cancer 2018;19:e109–e122. - PubMed
-
- Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet 2001;357:539–545. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
