

Using Epidemiological Data to Inform Clinical Trial Feasibility Assessments: A Case Study
- PMID: 36852687
- PMCID: PMC10050115
- DOI: 10.1161/STROKEAHA.122.041650
Using Epidemiological Data to Inform Clinical Trial Feasibility Assessments: A Case Study
Abstract
Background: Clinical trial enrollment and completion is challenging, with nearly half of all trials not being completed or not completed on time. In 2014, the National Institutes of Health StrokeNet in collaboration with stroke epidemiologists from GCNKSS (Greater Cincinnati/Northern Kentucky Stroke Study) began providing proposed clinical trials with formal trial feasibility assessments. Herein, we describe the process of prospective feasibility analyses using epidemiological data that can be used to improve enrollment and increase the likelihood a trial is completed.
Methods: In 2014, DEFUSE 3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trialists, National Institutes of Health StrokeNet, and stroke epidemiologists from GCNKSS collaborated to evaluate the initial inclusion/exclusion criteria for the DEFUSE 3 study. Trial criteria were discussed and an assessment was completed to evaluate the percent of the stroke population that might be eligible for the study. The DEFUSE 3 trial was stopped early with the publication of DAWN (Thrombectomy 6 to 24 Hours After Stroke With a Mismatch Between Deficit and Infarct), and the Wilcoxon rank-sum statistic was used to analyze whether the trial would have been stopped had the proposed changes not been made, following the DEFUSE 3 statistical analysis plan.
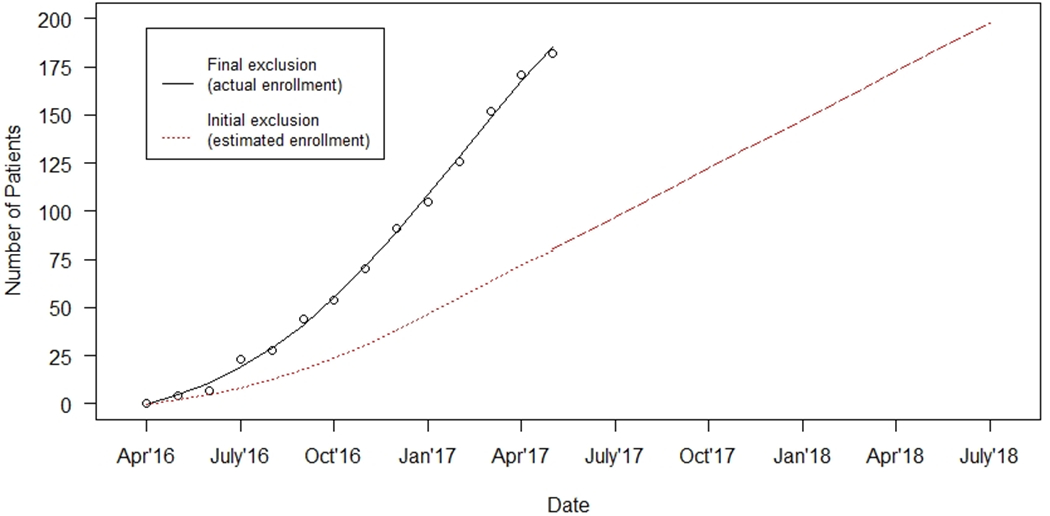
Results: After initial epidemiological analysis, 2.4% of patients with acute stroke in the GCNKSS population would have been predicted to be eligible for the study. After discussion with primary investigators and modifying 4 key exclusion criteria (upper limit of age increased to 90 years, baseline modified Rankin Scale broadened to 0-2, time since last well expanded to 16 hours, and decreased lower limit of National Institutes of Health Stroke Scale score to <6), the number predicted to be eligible for the trial increased to 4%. At the time of trial conclusion, 57% of the enrolled patients qualified only by the modified criteria, and the trial was stopped at an interim analysis that demonstrated efficacy. We estimated that the Wilcoxon rank-sum value for the unadjusted predicted enrollment would not have crossed the threshold for efficacy and the trial not stopped.
Conclusions: Objectively assessing trial inclusion/exclusion criteria using a population-based resource in a collaborative and iterative process including epidemiologists can lead to improved recruitment and can increase the likelihood of successful trial completion.
Keywords: clinical trial; epidemiologists; feasibility studies; ischemic stroke; prospective studies.
Figures
References
-
- Ehrhardt S, Appel LJ, Meinert CL. Trends in National Institutes of Health Funding for Clinical Trials Registered in ClinicalTrials.gov. JAMA. 2015;314:2566–2567. doi: 10.1001/jama.2015.12206 - DOI - PMC - PubMed
-
- Frank G Current challenges in clinical trial patient recruitment and enrollment. SoCRA Source. 2004;2:30–38.
