

Endovascular Ultrasound Renal Denervation to Treat Hypertension: The RADIANCE II Randomized Clinical Trial
- PMID: 36853250
- PMCID: PMC9975904
- DOI: 10.1001/jama.2023.0713
Endovascular Ultrasound Renal Denervation to Treat Hypertension: The RADIANCE II Randomized Clinical Trial
Erratum in
-
Two Incorrect Names.JAMA. 2023 Jun 13;329(22):1989. doi: 10.1001/jama.2023.8136. JAMA. 2023. PMID: 37314287 Free PMC article. No abstract available.
Abstract
Importance: Two initial sham-controlled trials demonstrated that ultrasound renal denervation decreases blood pressure (BP) in patients with mild to moderate hypertension and hypertension that is resistant to treatment.
Objective: To study the efficacy and safety of ultrasound renal denervation without the confounding influence of antihypertensive medications in patients with hypertension.
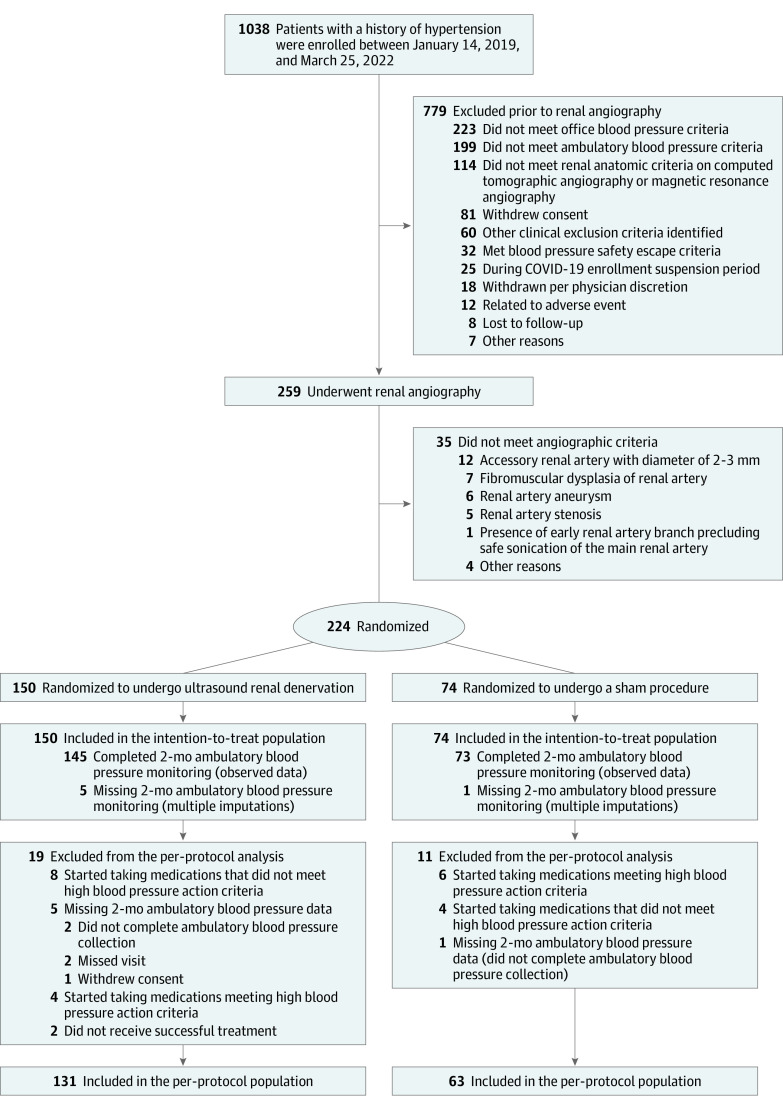
Design, setting, and participants: Sham-controlled, randomized clinical trial with patients and outcome assessors blinded to treatment assignment that was conducted between January 14, 2019, and March 25, 2022, at 37 centers in the US and 24 centers in Europe, with randomization stratified by center. Patients aged 18 years to 75 years with hypertension (seated office systolic BP [SBP] ≥140 mm Hg and diastolic BP [DBP] ≥90 mm Hg despite taking up to 2 antihypertensive medications) were eligible if they had an ambulatory SBP/DBP of 135/85 mm Hg or greater and an SBP/DBP less than 170/105 mm Hg after a 4-week washout of their medications. Patients with an estimated glomerular filtration rate of 40 mL/min/1.73 m2 or greater and with suitable renal artery anatomy were randomized 2:1 to undergo ultrasound renal denervation or a sham procedure. Patients were to abstain from antihypertensive medications until the 2-month follow-up unless prespecified BP criteria were exceeded and were associated with clinical symptoms.
Interventions: Ultrasound renal denervation vs a sham procedure.
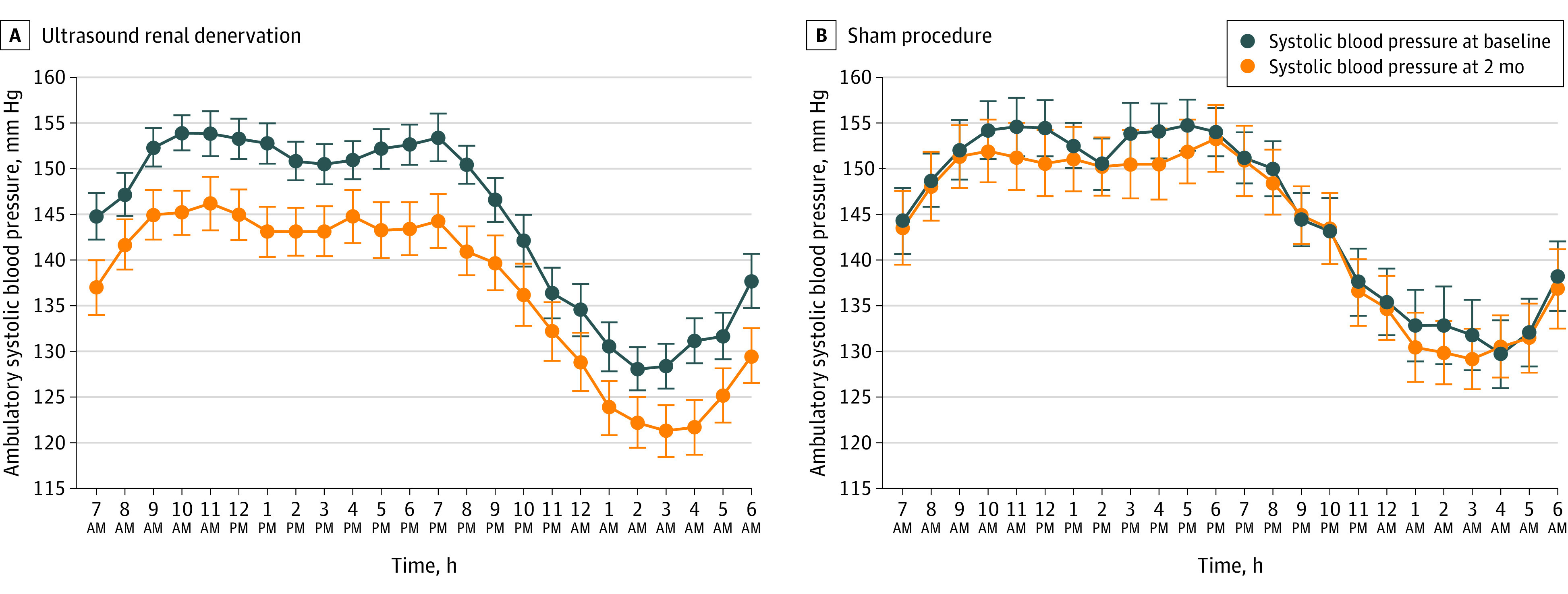
Main outcomes and measures: The primary efficacy outcome was the mean change in daytime ambulatory SBP at 2 months. The primary safety composite outcome of major adverse events included death, kidney failure, and major embolic, vascular, cardiovascular, cerebrovascular, and hypertensive events at 30 days and renal artery stenosis greater than 70% detected at 6 months. The secondary outcomes included mean change in 24-hour ambulatory SBP, home SBP, office SBP, and all DBP parameters at 2 months.
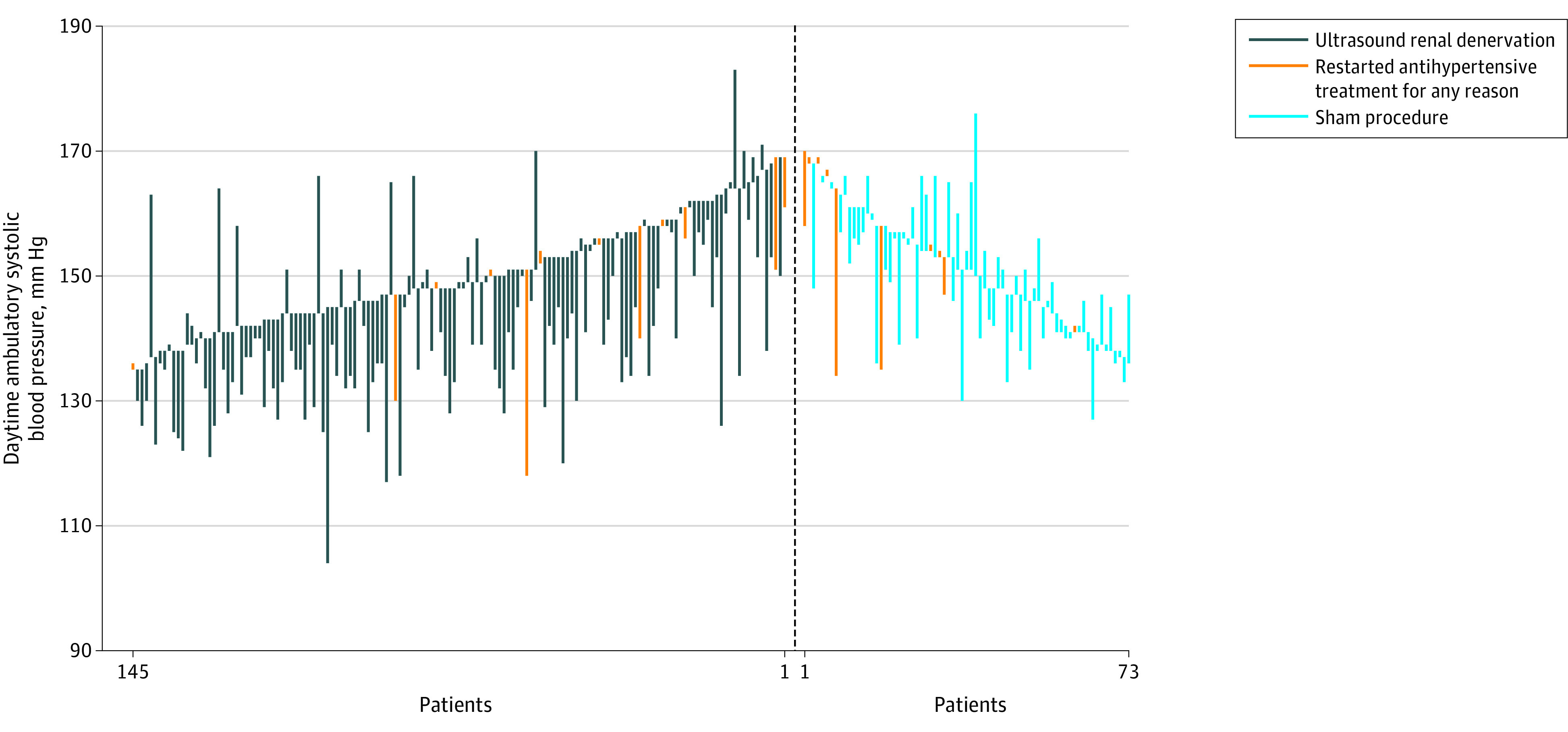
Results: Among 1038 eligible patients, 150 were randomized to ultrasound renal denervation and 74 to a sham procedure (mean age, 55 years [SD, 9.3 years]; 28.6% female; and 16.1% self-identified as Black or African American). The reduction in daytime ambulatory SBP was greater with ultrasound renal denervation (mean, -7.9 mm Hg [SD, 11.6 mm Hg]) vs the sham procedure (mean, -1.8 mm Hg [SD, 9.5 mm Hg]) (baseline-adjusted between-group difference, -6.3 mm Hg [95% CI, -9.3 to -3.2 mm Hg], P < .001), with a consistent effect of ultrasound renal denervation throughout the 24-hour circadian cycle. Among 7 secondary BP outcomes, 6 were significantly improved with ultrasound renal denervation vs the sham procedure. No major adverse events were reported in either group.
Conclusions and relevance: In patients with hypertension, ultrasound renal denervation reduced daytime ambulatory SBP at 2 months in the absence of antihypertensive medications vs a sham procedure without postprocedural major adverse events.
Trial registration: ClinicalTrials.gov Identifier: NCT03614260.
Conflict of interest statement
Figures
Comment in
-
In hypertension not treated with medications, renal denervation vs. sham reduced daytime ambulatory SBP at 2 mo.Ann Intern Med. 2023 Jun;176(6):JC68. doi: 10.7326/J23-0040. Epub 2023 Jun 6. Ann Intern Med. 2023. PMID: 37276593
References
-
- Zhou B, Carrillo-Larco RM, Danaei G, et al. ; NCD Risk Factor Collaboration (NCD-RisC) . Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957-980. doi: 10.1016/S0140-6736(21)01330-1 - DOI - PMC - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2018;138(17):e426-e483. doi: 10.1161/CIR.0000000000000597 - DOI - PubMed
-
- Choudhry NK, Kronish IM, Vongpatanasin W, et al. ; American Heart Association Council on Hypertension; Council on Cardiovascular and Stroke Nursing; and Council on Clinical Cardiology . Medication adherence and blood pressure control: a scientific statement from the American Heart Association. Hypertension. 2022;79(1):e1-e14. doi: 10.1161/HYP.0000000000000203 - DOI - PMC - PubMed
