

A phase 1 study of veliparib (ABT-888) plus weekly carboplatin and paclitaxel in advanced solid malignancies, with an expansion cohort in triple negative breast cancer (TNBC) (ETCTN 8620)
- PMID: 36853577
- PMCID: PMC10710035
- DOI: 10.1007/s10549-023-06889-0
A phase 1 study of veliparib (ABT-888) plus weekly carboplatin and paclitaxel in advanced solid malignancies, with an expansion cohort in triple negative breast cancer (TNBC) (ETCTN 8620)
Abstract
Background: Veliparib is a poly-ADP-ribose polymerase (PARP) inhibitor, and it has clinical activity with every 3 weeks carboplatin and paclitaxel. In breast cancer, weekly paclitaxel is associated with improved overall survival. We aimed to determine the maximum tolerated dose (MTD) and recommended phase 2 dose (RP2D) of veliparib with weekly carboplatin and paclitaxel as well as safety, pharmacokinetics, and preliminary clinical activity in triple negative breast cancer (TNBC).
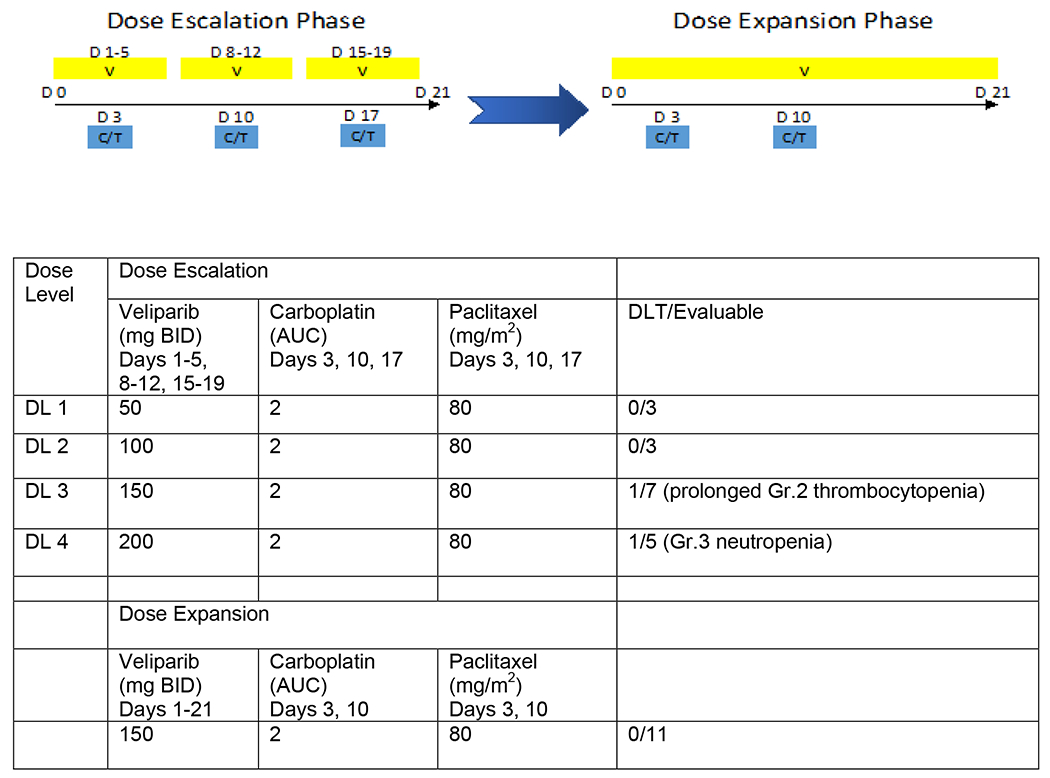
Methods: Patients with locally advanced/metastatic solid tumors and adequate organ function were eligible. A standard 3 + 3 dose-escalation design was followed by a TNBC expansion cohort. Veliparib doses ranging from 50 to 200 mg orally bid were tested with carboplatin (AUC 2) and paclitaxel (80 mg/m2) given weekly in a 21-day cycle. Adverse events (AE) were evaluated by CTCAE v4.0, and objective response rate (ORR) was determined by RECIST 1.1.
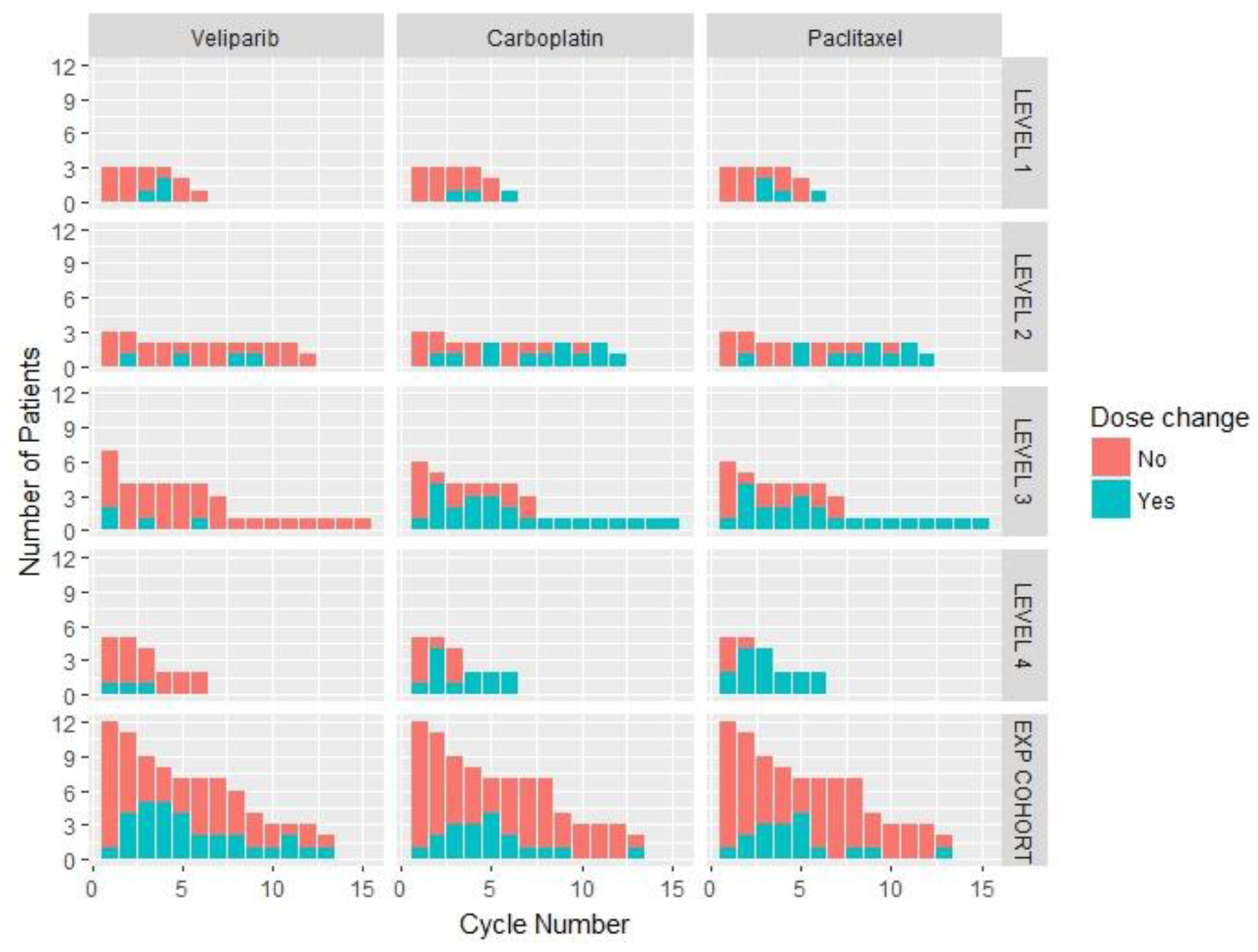
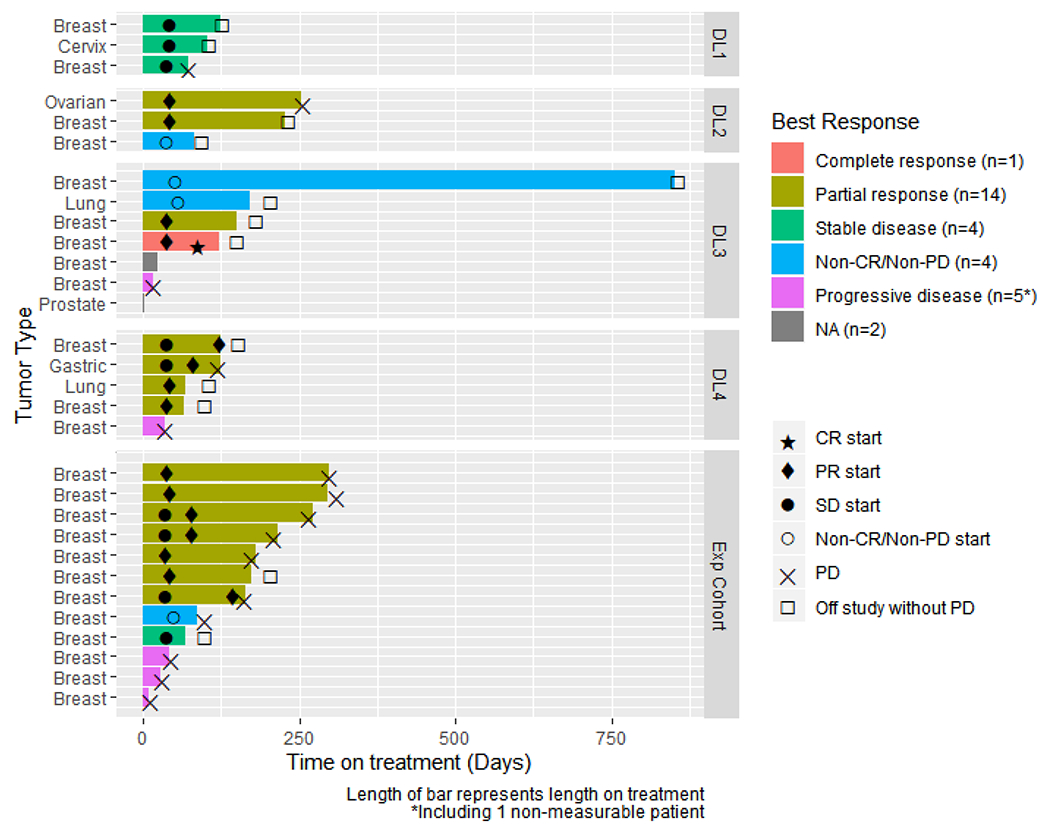
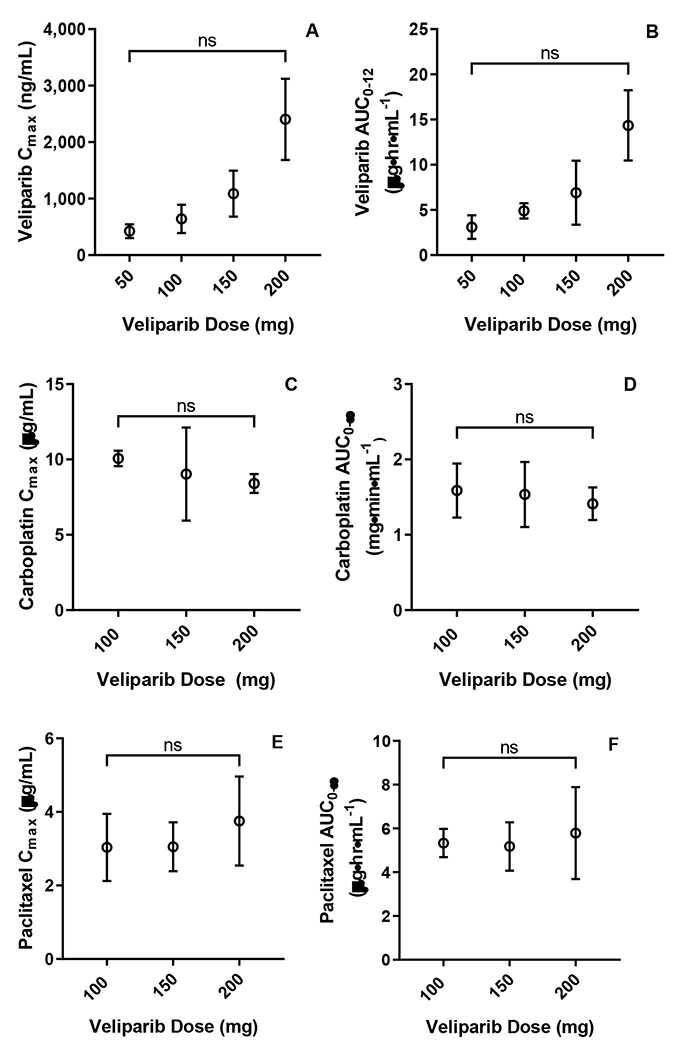
Results: Thirty patients were enrolled, of whom 22 had TNBC. Two dose-limiting toxicities were observed. The RP2D was determined to be 150 mg PO bid veliparib with weekly carboplatin and paclitaxel 2 weeks on, 1 week off, based on hematologic toxicity requiring dose reduction in the first 5 cycles of treatment. The most common grade 3/4 AEs included neutropenia, anemia, and thrombocytopenia. PK parameters of veliparib were comparable to single-agent veliparib. In 23 patients with evaluable disease, the ORR was 65%. In 19 patients with TNBC with evaluable disease, the ORR was 63%.
Conclusion: Veliparib can be safely combined with weekly paclitaxel and carboplatin, and this triplet combination has promising clinical activity.
Keywords: DNA damage; PARP; Pharmacokinetics; Phase 1 study; Solid tumors; Triple negative breast cancer; Veliparib.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Jan Beumer’s institute received research support from AbbVie. Leisha Emens has received research support from Aduro Biotech, AstraZeneca, Breast Cancer Research Foundation, Corvus, Department of Defense, EMD Serono, Genentech, HeritX, Inc., Maxcyte, Merck, National Cancer Institute, NSABP Foundation, Roche, Translational Breast Cancer Research Consortium, and has served as a consultant for AbbVie, Amgen, AstraZeneca, Bayer, Bristol-Myers Squibb, Celgene, Genentech, Gritstone, Lilly, Macrogenics, Medimmune, Molecuvax, Novartis, Peregrine, Replimune, Roche, Syndax, and Vaccinex. She has also received royalties from Aduro Biotech. Shannon Puhalla has received research support from AbbVie, Pfizer, Lilly, Novartis, Incyte, Covance-Bayer, AstraZeneca, Genentech, Medivation and has been a consultant for AbbVie, MedImmune, Celldex, Puma, Pfizer, AstraZeneca, Esai, and Nanostring. Stacie Shepherd is a former employee of Abbott, AbbVie, and Corcept and holds Abbott, AbbVie, and Corcept stocks.
Figures
References
-
- Foulkes WD, Brunet JS, Stefansson IM, Straume O, Chappuis PO, Begin LR, Hamel N, Goffin JR, Wong N, Trudel M et al. : The prognostic implication of the basal-like (cyclin E high/p27 low/p53+/glomeruloid-microvascular-proliferation+) phenotype of BRCA1-related breast cancer. Cancer research 2004, 64(3):830–835. - PubMed
-
- Lakhani SR, Van De Vijver MJ, Jacquemier J, Anderson TJ, Osin PP, McGuffog L, Easton DF: The pathology of familial breast cancer: predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2002, 20(9):2310–2318. - PubMed
-
- Isakoff SJ, Mayer EL, He L, Traina TA, Carey LA, Krag KJ, Rugo HS, Liu MC, Stearns V, Come SE et al. : TBCRC009: A Multicenter Phase II Clinical Trial of Platinum Monotherapy With Biomarker Assessment in Metastatic Triple-Negative Breast Cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2015, 33(17):1902–1909. - PMC - PubMed
-
- Vos S, van Diest PJ, Moelans CB: A systematic review on the frequency of BRCA promoter methylation in breast and ovarian carcinomas of BRCA germline mutation carriers: Mutually exclusive, or not? Critical reviews in oncology/hematology 2018, 127:29–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
