

Higher Surgeon Volume is Associated With a Lower Rate of Subsequent Revision Procedures After Total Shoulder Arthroplasty: A National Analysis
- PMID: 36853863
- PMCID: PMC10344546
- DOI: 10.1097/CORR.0000000000002605
Higher Surgeon Volume is Associated With a Lower Rate of Subsequent Revision Procedures After Total Shoulder Arthroplasty: A National Analysis
Abstract
Background: Studies assessing the relationship between surgeon volume and outcomes have shown mixed results, depending on the specific procedure analyzed. This volume relationship has not been well studied in patients undergoing total shoulder arthroplasty (TSA), but it should be, because this procedure is common, expensive, and potentially morbid.
Questions/purposes: We performed this study to assess the association between increasing surgeon volume and decreasing rate of revision at 2 years for (1) anatomic TSA (aTSA) and (2) reverse TSA (rTSA) in the United States.
Methods: In this retrospective study, we used Centers for Medicare and Medicaid Services (CMS) fee-for-service inpatient and outpatient data from 2015 to 2021 to study the association between annual surgeon aTSA and rTSA volume and 2-year revision shoulder procedures after the initial surgery. The CMS database was chosen for this study because it is a national sample and can be used to follow patients over time. We included patients with Diagnosis-related Group code 483 and Current Procedural Terminology code 23472 for TSA (these codes include both aTSA and rTSA). We used International Classification of Diseases, Tenth Revision, procedural codes. Patients who underwent shoulder arthroplasty for fracture (10% [17,524 of 173,242]) were excluded. We studied the variables associated with the subsequent procedure rate through a generalized linear model, controlling for confounders such as patient age, comorbidity risk score, surgeon and hospital volume, surgeon graduation year, hospital size and teaching status, assuming a binomial distribution with the dependent variable being whether an episode had at least one subsequent procedure within 2 years. The regression was fitted with standard errors clustered at the hospital level, combining all TSAs and within the aTSA and rTSA groups, respectively. Hospital and surgeon yearly volumes were calculated by including all TSAs, primary procedure and subsequent, during the study period. Other hospital-level and surgeon-level characteristics were obtained through public files from the CMS. The CMS Hierarchical Condition Category risk score was controlled because it is a measure reflecting the expected future health costs for each patient based on the patient's demographics and chronic illnesses. We then converted regression coefficients to the percentage change in the odds of having a subsequent procedure.
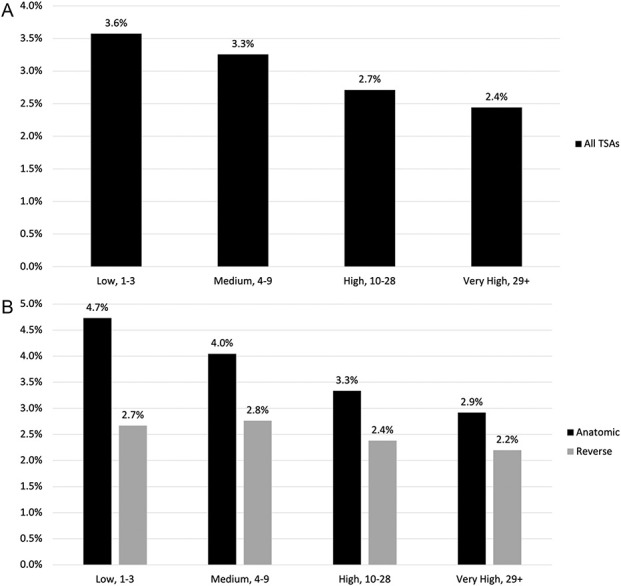
Results: After controlling for confounding variables including patient age, comorbidity risk score, surgeon and hospital volume, surgeon graduation year, and hospital size and teaching status, we found that an annual surgeon volume of ≥ 10 aTSAs was associated with a 27% decreased odds of revision within 2 years (95% confidence interval 13% to 39%; p < 0.001), while surgeon volume of ≥ 29 aTSAs was associated with a 33% decreased odds of revision within 2 years (95% CI 18% to 45%; p < 0.001) compared with a volume of fewer than four aTSAs per year. Annual surgeon volume of ≥ 29 rTSAs was associated with a 26% decreased odds of revision within 2 years (95% CI 9% to 39%; p < 0.001).
Conclusion: Surgeons should consider modalities such as virtual planning software, templating, or enhanced surgeon training to aid lower-volume surgeons who perform aTSA and rTSA. More research is needed to assess the value of these modalities and their relationship with the rates of subsequent revision.
Level of evidence: Level III, therapeutic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures


Comment in
-
CORR Insights®: Higher Surgeon Volume is Associated With a Lower Rate of Subsequent Revision Procedures After Total Shoulder Arthroplasty: A National Analysis.Clin Orthop Relat Res. 2023 Aug 1;481(8):1581-1582. doi: 10.1097/CORR.0000000000002654. Epub 2023 Apr 4. Clin Orthop Relat Res. 2023. PMID: 37017591 Free PMC article. No abstract available.
References
-
- Battaglia T, Mulhall K, Brown T, Saleh K. Increased surgical volume is associated with lower THA dislocation rates. Clin Orthop Relat Res. 2006;447:28-33. - PubMed
-
- Best MJ, Aziz KT, Wilckens JH, McFarland EG, Srikumaran U. Increasing incidence of primary reverse and anatomic total shoulder arthroplasty in the United States. J Shoulder Elbow Surg. 2021;30:1159-1166. - PubMed
-
- Brown JS, Gordon RJ, Peng Y, Hatton A, Page RS, Macgroarty KA. Lower operating volume in shoulder arthroplasty is associated with increased revision rates in the early postoperative period: long-term analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Shoulder Elbow Surg. 2020;29:1104-1114. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
