

Prescribing, deprescribing and potential adverse effects of proton pump inhibitors in older patients with multimorbidity: an observational study
- PMID: 36854455
- PMCID: PMC9981164
- DOI: 10.9778/cmajo.20210240
Prescribing, deprescribing and potential adverse effects of proton pump inhibitors in older patients with multimorbidity: an observational study
Abstract
Background: Proton pump inhibitors (PPIs) contribute to polypharmacy and are associated with adverse effects. As prospective data on longitudinal patterns of PPI prescribing in older patients with multimorbidity are lacking, we sought to assess patterns of PPI prescribing and deprescribing, as well as the association of PPI use with hospital admissions over 1 year in this population.
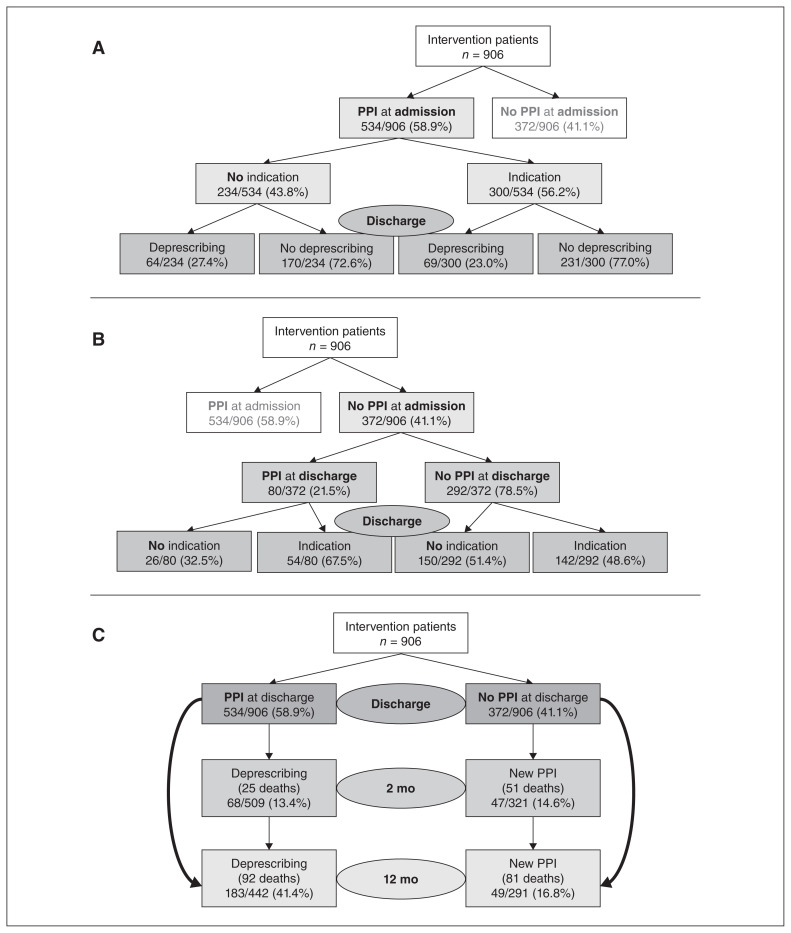
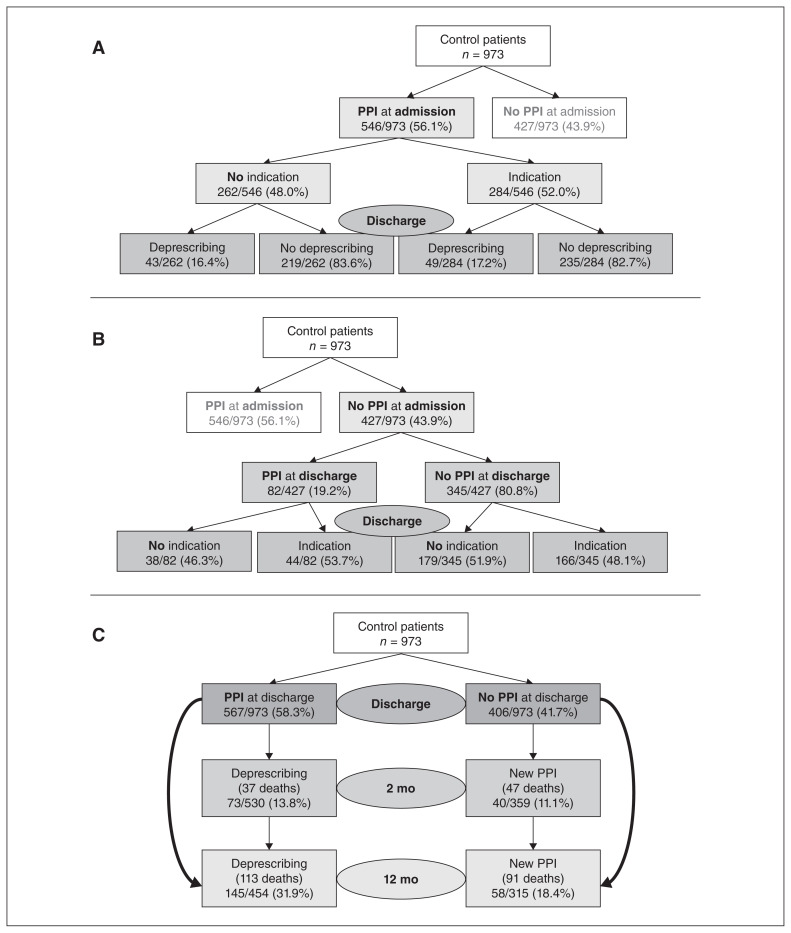
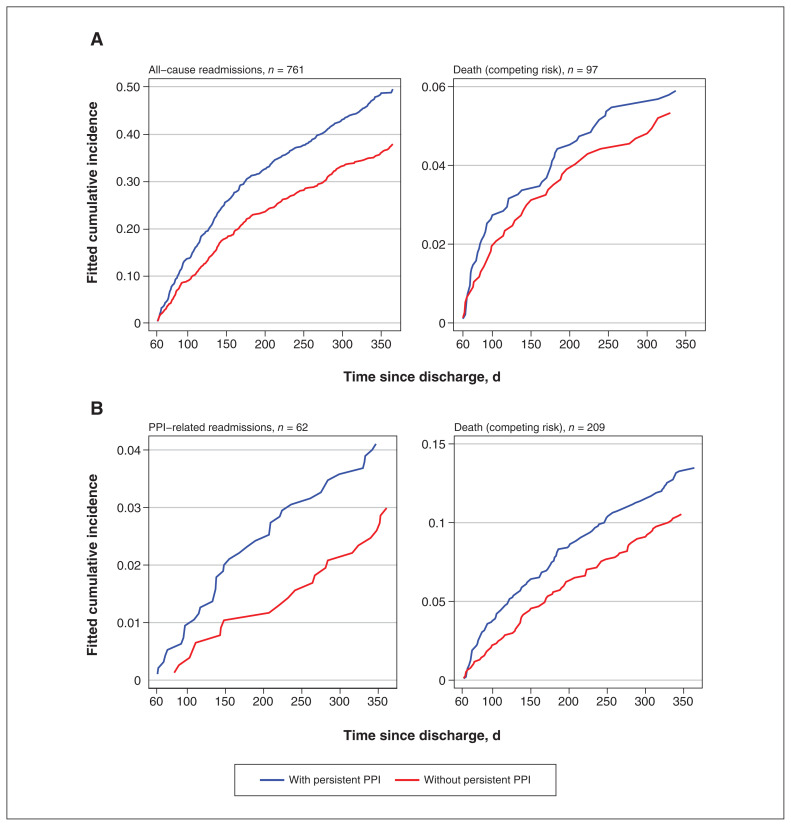
Methods: We conducted a prospective, longitudinal cohort study using data from the Optimizing Therapy to Prevent Avoidable Hospital Admissions in Multimorbid Older Adults (OPERAM) trial, a randomized controlled trial testing an intervention to reduce inappropriate prescribing (2016-2018). This trial included adults aged 70 years and older with at least 3 chronic conditions and prescribed at least 5 chronic medications. We assessed prevalence of PPI use at time of hospital admission, and new prescriptions and deprescribing at discharge, and at 2 months and 1 year after discharge, by intervention group. We used a regression with competing risk for death to assess the association of PPI use with readmissions related to their potential adverse effects, and all-cause readmission.
Results: Overall, 1080 (57.4%) of 1879 patients (mean age 79 yr) had PPI prescriptions at admission, including 496 (45.9%) patients with a potentially inappropriate indication. At discharge, 133 (24.9%) of 534 patients in the intervention group and 92 (16.8%) of 546 patients in the control group who were using PPIs at admission had deprescribing. Among 680 patients who were not using PPIs at discharge, 47 (14.6%) of 321 patients in the intervention group and 40 (11.1%) of 359 patients in the control group had a PPI started within 2 months. Use of PPIs was associated with all-cause readmission (n = 770, subdistribution hazard ratio 1.31, 95% confidence interval 1.12-1.53).
Interpretation: Potentially inappropriate use of PPI, new PPI prescriptions and PPI deprescribing were frequent among older adults with multimorbidity and polypharmacy. These data suggest that persistent PPI use may be associated with clinically important adverse effects in this population.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
DepRescribing inapprOpriate Proton Pump InhibiTors (DROPIT): study protocol of a cluster-randomised controlled trial in Swiss primary care.BMJ Open. 2025 Jan 20;15(1):e094495. doi: 10.1136/bmjopen-2024-094495. BMJ Open. 2025. PMID: 39832992 Free PMC article.
-
Effectiveness of a multi-faceted intervention to deprescribe proton pump inhibitors in primary care: protocol for a population-based, pragmatic, cluster-randomized controlled trial.BMC Health Serv Res. 2022 Feb 17;22(1):219. doi: 10.1186/s12913-022-07496-3. BMC Health Serv Res. 2022. PMID: 35177042 Free PMC article.
-
Development and Implementation of a Pharmacist-Led Proton Pump Inhibitor Deprescribing Algorithm in a Geriatric Ambulatory Office.Sr Care Pharm. 2023 Mar 1;38(3):105-112. doi: 10.4140/TCP.n.2023.105. Sr Care Pharm. 2023. PMID: 36803698
-
Problems Associated with Deprescribing of Proton Pump Inhibitors.Int J Mol Sci. 2019 Nov 2;20(21):5469. doi: 10.3390/ijms20215469. Int J Mol Sci. 2019. PMID: 31684070 Free PMC article. Review.
-
Inappropriate polypharmacy management versus deprescribing: A review on their relationship.Basic Clin Pharmacol Toxicol. 2024 Jan;134(1):6-14. doi: 10.1111/bcpt.13920. Epub 2023 Jul 11. Basic Clin Pharmacol Toxicol. 2024. PMID: 37350370 Review.
Cited by
-
Proton Pump Inhibitors: Rational Use and Use-Reduction - The Windsor Workshop.Dig Dis. 2024;42(3):211-220. doi: 10.1159/000538399. Epub 2024 Mar 21. Dig Dis. 2024. PMID: 38513623 Free PMC article. Review.
-
Association between proton pump inhibitors and risk of hepatic encephalopathy in patients undergoing transjugular intrahepatic portosystemic shunt: a protocol for a systematic review and meta-analysis.BMJ Open. 2024 Apr 2;14(4):e078412. doi: 10.1136/bmjopen-2023-078412. BMJ Open. 2024. PMID: 38569689 Free PMC article.
-
Approaches to Deprescribing Proton Pump Inhibitors in Clinical Practice: A Systematic Review.J Clin Med. 2024 Oct 21;13(20):6283. doi: 10.3390/jcm13206283. J Clin Med. 2024. PMID: 39458232 Free PMC article. Review.
-
Proton Pump Inhibitors in Germany: Status Quo of a Growing Market.Health Serv Res Manag Epidemiol. 2024 Apr 1;11:23333928241241220. doi: 10.1177/23333928241241220. eCollection 2024 Jan-Dec. Health Serv Res Manag Epidemiol. 2024. PMID: 38562150 Free PMC article.
-
Determinants of and interventions for Proton Pump Inhibitor prescription behavior: A systematic scoping review.BMC Prim Care. 2024 Jun 11;25(1):208. doi: 10.1186/s12875-024-02459-5. BMC Prim Care. 2024. PMID: 38862886 Free PMC article.
References
-
- Masclee GMC, Sturkenboom MCJM, Kuipers EJ. A benefit-risk assessment of the use of proton pump inhibitors in the elderly. Drugs Aging. 2014;31:263–82. - PubMed
-
- Nehra AK, Alexander JA, Loftus CG, et al. Proton pump inhibitors: review of emerging concerns. Mayo Clin Proc. 2018;93:240–6. - PubMed
-
- Pham CQD, Regal RE, Bostwick TR, et al. Acid suppressive therapy use on an inpatient internal medicine service. Ann Pharmacother. 2006;40:1261–6. - PubMed
-
- Thomas L, Culley EJ, Gladowski P, et al. Longitudinal analysis of the costs associated with inpatient initiation and subsequent outpatient continuation of proton pump inhibitor therapy for stress ulcer prophylaxis in a large managed care organization. J Manag Care Pharm. 2010;16:122–9. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials