

Characterisation of medical conditions of children with sickle cell disease in the USA: findings from the 2007-2018 National Health Interview Survey (NHIS)
- PMID: 36854589
- PMCID: PMC9980332
- DOI: 10.1136/bmjopen-2022-069075
Characterisation of medical conditions of children with sickle cell disease in the USA: findings from the 2007-2018 National Health Interview Survey (NHIS)
Abstract
Objectives: We used the National Health Interview Survey (NHIS) data set to examine the prevalence of comorbid medical conditions; explore barriers to accessing healthcare and special educational services; and assess the associations between sickle cell disease (SCD) status and demographics/socioeconomic status (SES), and social determinants of health (SDoH) on comorbidities among children in the USA.
Design: Cross-sectional.
Setting: NHIS Sample Child Core questionnaire 2007-2018 data set.
Participants: 133 481 children; presence of SCD was determined by an affirmative response from the adult or guardian of the child.
Main outcome measures: Multivariate logistic regression was used to compare the associations between SCD status, SES and SDoH for various medical conditions for all races and separately for black children at p<0.05.
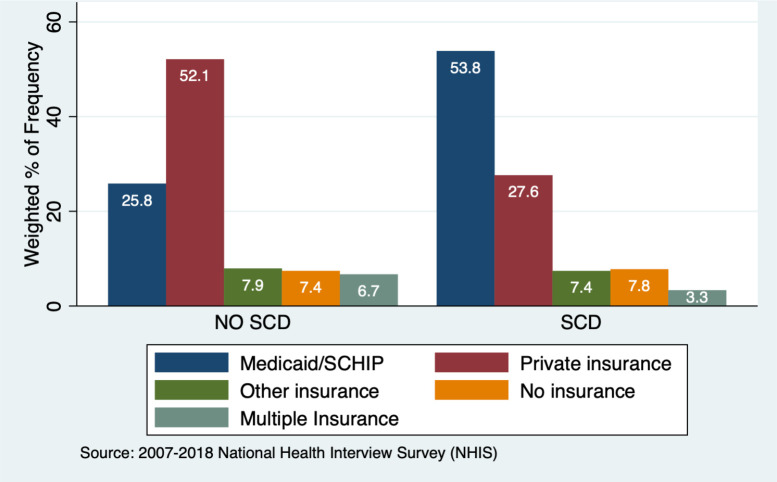
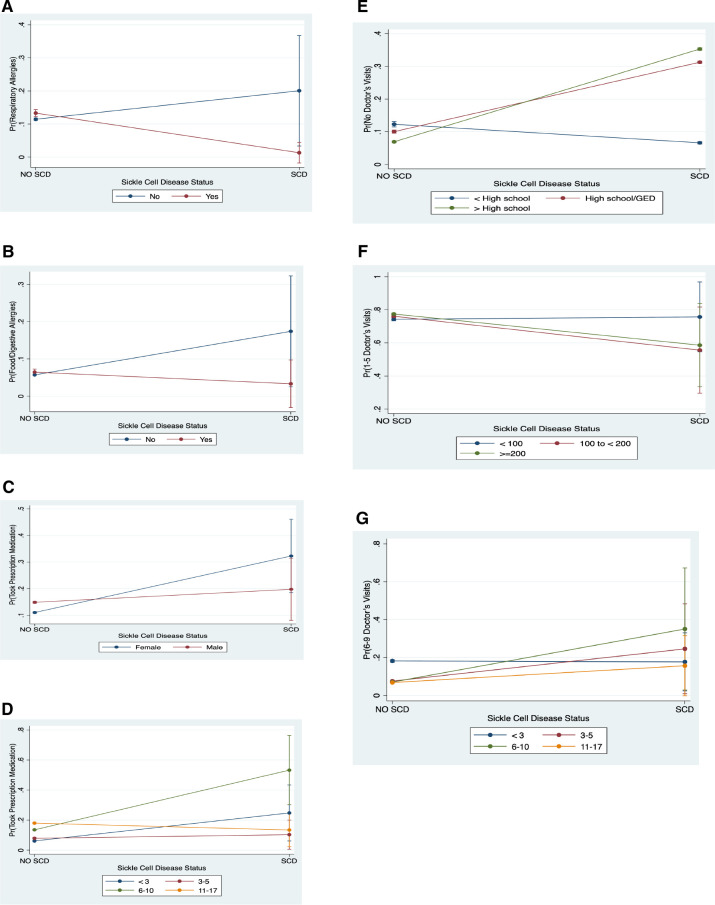
Results: 133 481 children (mean age 8.5 years, SD: 0.02), 215 had SCD and ~82% (weighted) of the children with SCD are black. Children with SCD were more likely to suffer from comorbid conditions, that is, anaemia (adjusted OR: 27.1, p<0.001). Furthermore, children with SCD had at least two or more emergency room (ER) visits (p<0.001) and were more likely to have seen a doctor 1-15 times per year (p<0.05) compared with children without SCD. Household income (p<0.001) and maternal education were lower for children with SCD compared with children without SCD (52.4% vs 63.5% (p<0.05)). SCD children with a maternal parent who has < / > High School degree were less likely to have no ER visits or 4-5 ER visits, and more likely to have 2-3 ER visits within 12 months.
Conclusion: Children with SCD experienced significant comorbid conditions and have high healthcare usage, with black children being disproportionately affected. Moreover, maternal education status and poverty level illustrates how impactful SES can be on healthcare seeking behaviour for the SCD population. SDoH have significant implications for managing paediatric patients with SCD in clinical settings.
Keywords: anaemia; community child health; public health.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical