

Computed tomography derived cervical fat-free muscle fraction as an imaging-based outcome marker in patients with acute ischemic stroke: a pilot study
- PMID: 36855093
- PMCID: PMC9971678
- DOI: 10.1186/s12883-023-03132-7
Computed tomography derived cervical fat-free muscle fraction as an imaging-based outcome marker in patients with acute ischemic stroke: a pilot study
Abstract
Background: Outcome assessment in stroke patients is essential for evidence-based stroke care planning. Computed tomography (CT) is the mainstay of diagnosis in acute stroke. This study aimed to investigate whether CT-derived cervical fat-free muscle fraction (FFMF) as a biomarker of muscle quality is associated with outcome parameters after acute ischemic stroke.
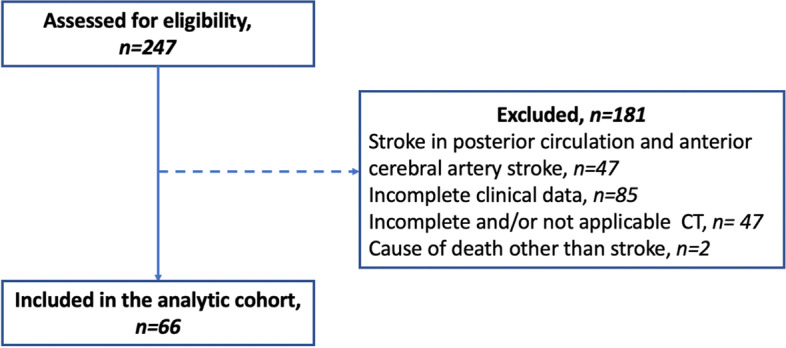
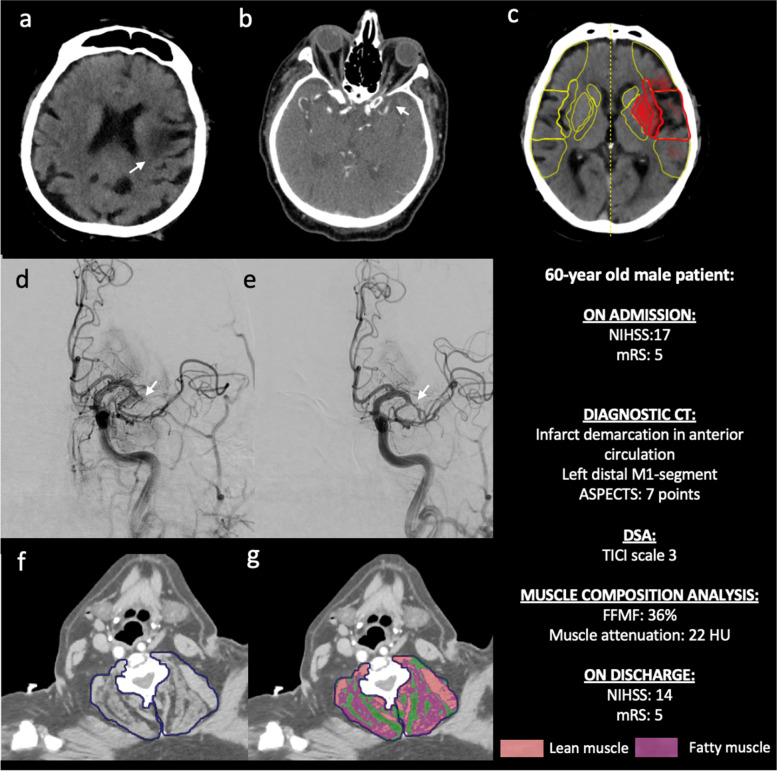
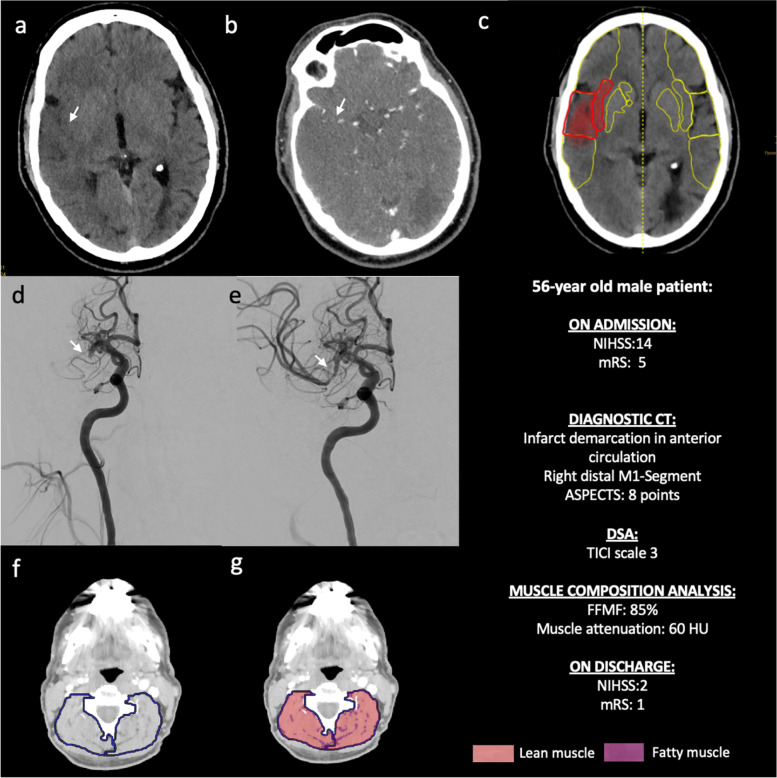
Methods: In this retrospective study, 66 patients (mean age: 76 ± 13 years, 30 female) with acute ischemic stroke in the anterior circulation who underwent CT, including CT-angiography, and endovascular mechanical thrombectomy of the middle cerebral artery between August 2016 and January 2020 were identified. Based on densitometric thresholds, cervical paraspinal muscles covered on CT-angiography were separated into areas of fatty and lean muscle and FFMF was calculated. The study cohort was binarized based on median FFMF (cutoff value: < 71.6%) to compare clinical variables and outcome data between two groups. Unpaired t test and Mann-Whitney U test were used for statistical analysis.
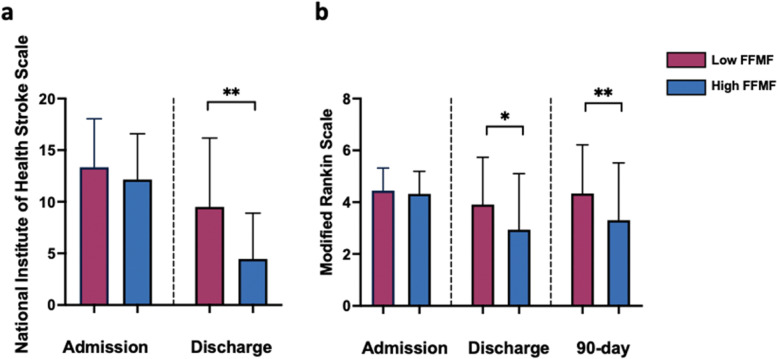
Results: National Institute of Health Stroke Scale (NIHSS) (12.2 ± 4.4 vs. 13.6 ± 4.5, P = 0.297) and modified Rankin scale (mRS) (4.3 ± 0.9 vs. 4.4 ± 0.9, P = 0.475) at admission, and pre-stroke mRS (1 ± 1.3 vs. 0.9 ± 1.4, P = 0.489) were similar between groups with high and low FFMF. NIHSS and mRS at discharge were significantly better in patients with high FFMF compared to patients with low FFMF (NIHSS: 4.5 ± 4.4 vs. 9.5 ± 6.7; P = 0.004 and mRS: 2.9 ± 2.1 vs.3.9 ± 1.8; P = 0.049). 90-day mRS was significantly better in patients with high FFMF compared to patients with low FFMF (3.3 ± 2.2 vs. 4.3 ± 1.9, P = 0.045).
Conclusion: Cervical FFMF obtained from routine clinical CT might be a new imaging-based muscle quality biomarker for outcome prediction in stroke patients.
Keywords: Acute ischemic stroke; Computed tomography; Fat-free muscle fraction; Muscle quality.
© 2023. The Author(s).
Conflict of interest statement
C.K. and J.R. are members of the European Reference Network on Rare Neuromuscular Diseases ERN EURO-NMD. ERN EURO-NMD had no influence on study conceptualization and design, collection and analysis of the data, manuscript preparation as well as the decision to publish. The remaining authors have no competing interests to declare that are relevant to the content of this article.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
