

The effect of metabolic dysfunction-associated fatty liver disease and diabetic kidney disease on the risk of hospitalization of heart failure in type 2 diabetes: a retrospective cohort study
- PMID: 36855144
- PMCID: PMC9976518
- DOI: 10.1186/s13098-023-01006-z
The effect of metabolic dysfunction-associated fatty liver disease and diabetic kidney disease on the risk of hospitalization of heart failure in type 2 diabetes: a retrospective cohort study
Abstract
Background: Diabetes mellitus is a major risk factor for heart failure. A recent consensus statement recommended annual cardiac biomarker testing (e.g. natriuretic peptide or high-sensitivity cardiac troponin) for all patients with diabetes. We aimed to identify patients at a higher risk of hospitalization for heart failure among patients with type 2 diabetes to prioritize those who would require screening.
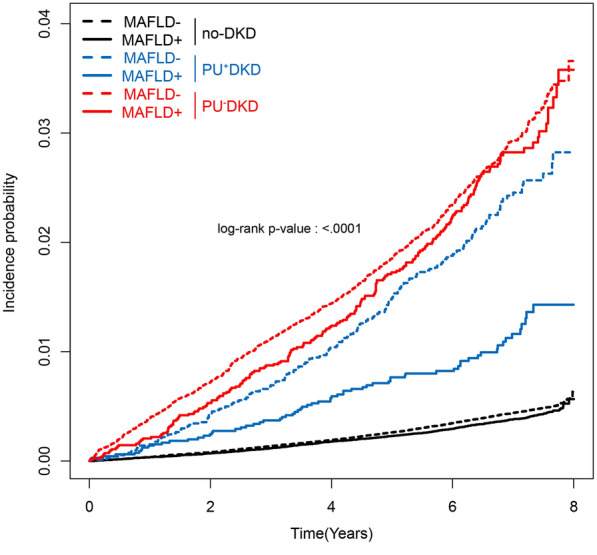
Methods: Overall, 1,189,113 patients who underwent two medical health checkup cycles (2009-2012 and 2011-2014) and had stable diabetic kidney disease (DKD) phenotype in the Korean National Health Insurance Service database were included in this study. After excluding those with concurrent proteinuria (PU) and reduced estimated glomerular filtration rate, three groups (no-DKD, PU+DKD, and PU-DKD) were identified. A fatty liver index of ≥ 60 was defined as metabolic dysfunction-associated fatty liver disease (MAFLD). Patients were followed up until December 2018 or until outcomes developed. The Cox proportional hazard model was used to compare the risk of hospitalization for heart failure across groups.
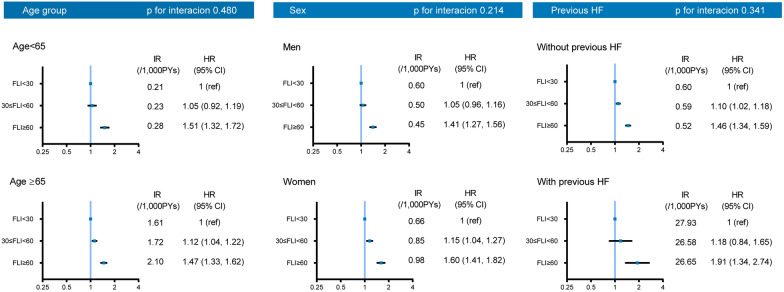
Results: During an average of 6.6 years of follow-up, 5781 patients developed hospitalization for heart failure. After adjusting for covariates, the risk of hospitalization for heart failure was highest in the PU+DKD group [HR 3.12, 95% CI (2.75-3.55)], followed by the PU-DKD group [HR 1.85, 95% CI (1.73-1.99)] using the no-DKD group as the reference category. The risk of hospitalization for heart failure was comparable regardless of MAFLD status in patients who already had DKD. However, in the no-DKD group, the risk of hospitalization for heart failure was 1.4 times higher in patients with MAFLD than in those without [HR 1.41, 95% CI (1.31-1.52)].
Conclusions: In lines with the international consensus statement, we suggest that annual cardiac biomarker testing should be conducted at least in patients with DKD and/or MAFLD.
Keywords: Diabetic kidney disease; Heart failure; Hospitalization for heart failure; Metabolic dysfunction–associated fatty liver disease.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Two-Year Changes in Diabetic Kidney Disease Phenotype and the Risk of Heart Failure: A Nationwide Population-Based Study in Korea.Diabetes Metab J. 2023 Jul;47(4):523-534. doi: 10.4093/dmj.2022.0096. Epub 2023 Apr 25. Diabetes Metab J. 2023. PMID: 37096376 Free PMC article.
-
Hip Fracture Risk According to Diabetic Kidney Disease Phenotype in a Korean Population.Endocrinol Metab (Seoul). 2022 Feb;37(1):148-158. doi: 10.3803/EnM.2021.1315. Epub 2022 Feb 28. Endocrinol Metab (Seoul). 2022. PMID: 35255607 Free PMC article.
-
Nonalbuminuric Diabetic Kidney Disease and Risk of All-Cause Mortality and Cardiovascular and Kidney Outcomes in Type 2 Diabetes: Findings From the Hong Kong Diabetes Biobank.Am J Kidney Dis. 2022 Aug;80(2):196-206.e1. doi: 10.1053/j.ajkd.2021.11.011. Epub 2022 Jan 6. Am J Kidney Dis. 2022. PMID: 34999159
-
Significance of Diabetic Kidney Disease Biomarkers in Predicting Metabolic-Associated Fatty Liver Disease.Biomedicines. 2023 Jul 7;11(7):1928. doi: 10.3390/biomedicines11071928. Biomedicines. 2023. PMID: 37509567 Free PMC article. Review.
-
Comparison of Nonalbuminuric and Albuminuric Diabetic Kidney Disease Among Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis.Front Endocrinol (Lausanne). 2022 Jun 3;13:871272. doi: 10.3389/fendo.2022.871272. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35721745 Free PMC article.
Cited by
-
Effects of APOE isoforms in diabetic nephropathy patients of South India.Acta Diabetol. 2025 Apr;62(4):487-497. doi: 10.1007/s00592-024-02374-2. Epub 2024 Oct 17. Acta Diabetol. 2025. PMID: 39417844 Free PMC article.
-
Metabolic Dysfunction Associated-Steatotic Liver Disease (MASLD) and Cardiovascular Risk: Embrace All Facets of the Disease.Curr Cardiol Rep. 2025 Jan 13;27(1):19. doi: 10.1007/s11886-024-02181-9. Curr Cardiol Rep. 2025. PMID: 39804409 Review.
-
Biomarker for cardiorenal syndrome risk in patients with liver cirrhosis and type 2 diabetes in Saudi Arabia.Saudi Med J. 2024 Jul;45(7):675-684. doi: 10.15537/smj.2024.45.7.20240156. Saudi Med J. 2024. PMID: 38955454 Free PMC article.
-
Salvianolic acid B ameliorates myocardial fibrosis in diabetic cardiomyopathy by deubiquitinating Smad7.Chin Med. 2023 Dec 10;18(1):161. doi: 10.1186/s13020-023-00868-9. Chin Med. 2023. PMID: 38072948 Free PMC article.
References
LinkOut - more resources
Full Text Sources
