

Morrison's Pouch: Anatomy and Radiological Appearance of Pathological Processes
- PMID: 36855710
- PMCID: PMC9968550
- DOI: 10.1055/s-0042-1758874
Morrison's Pouch: Anatomy and Radiological Appearance of Pathological Processes
Abstract
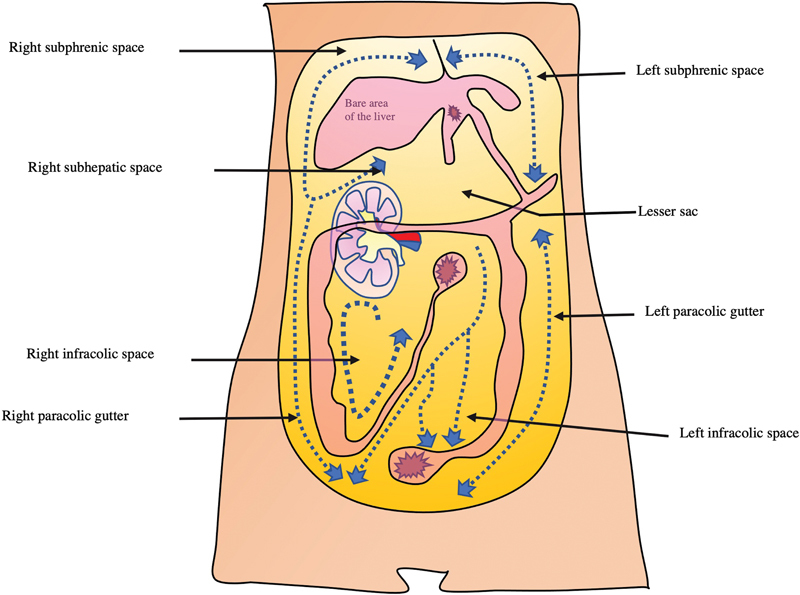
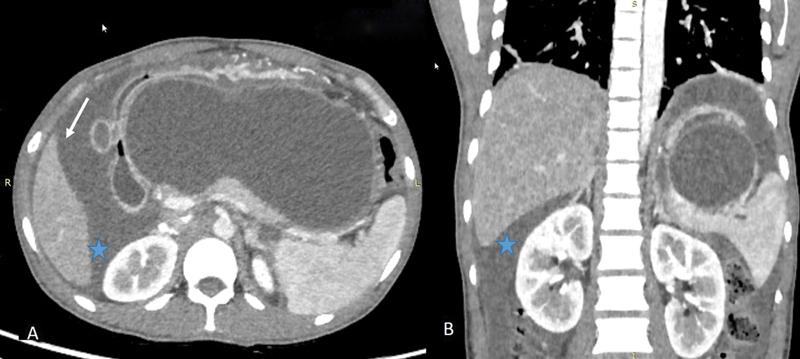
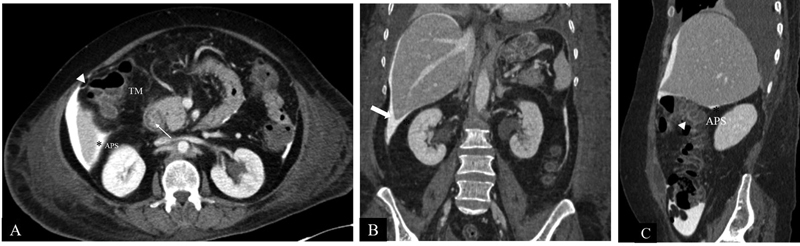
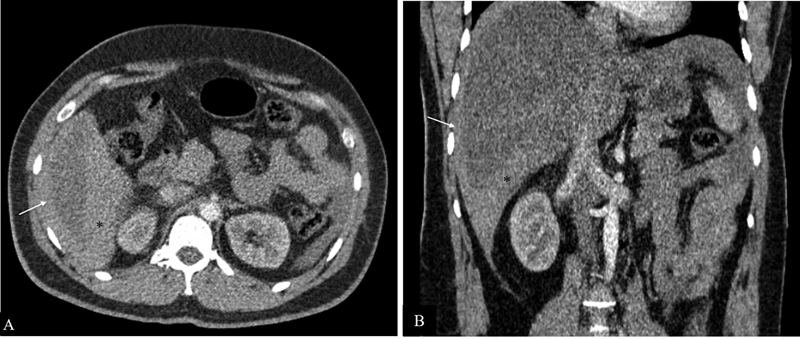
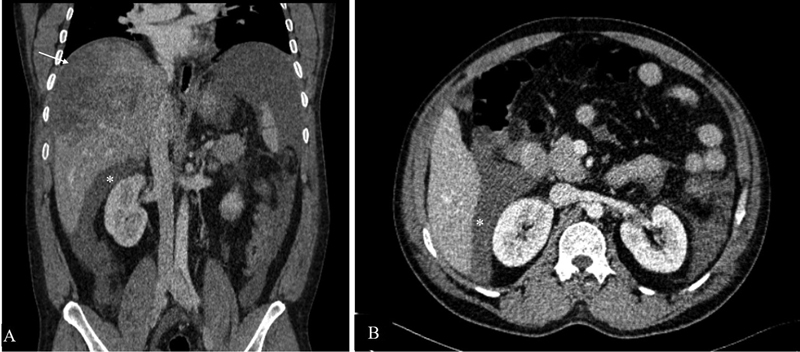
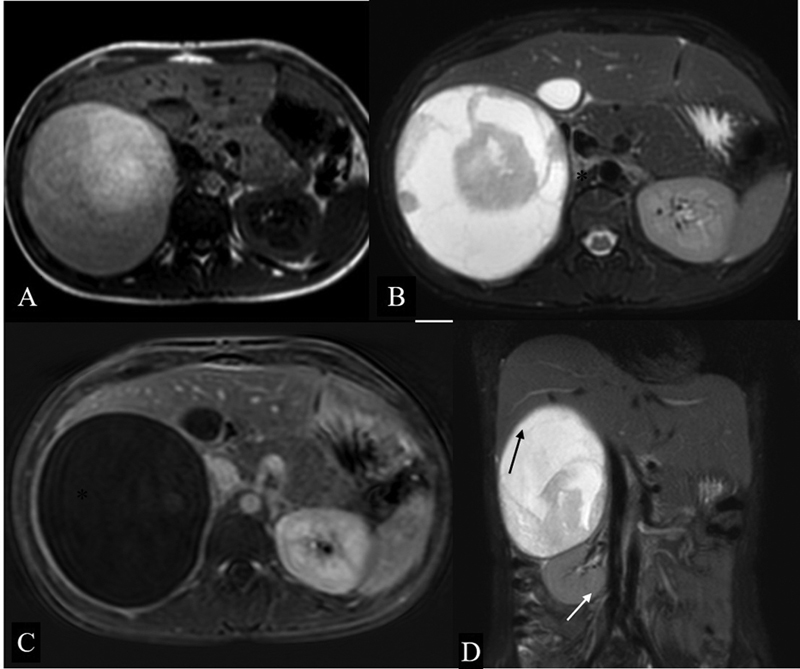
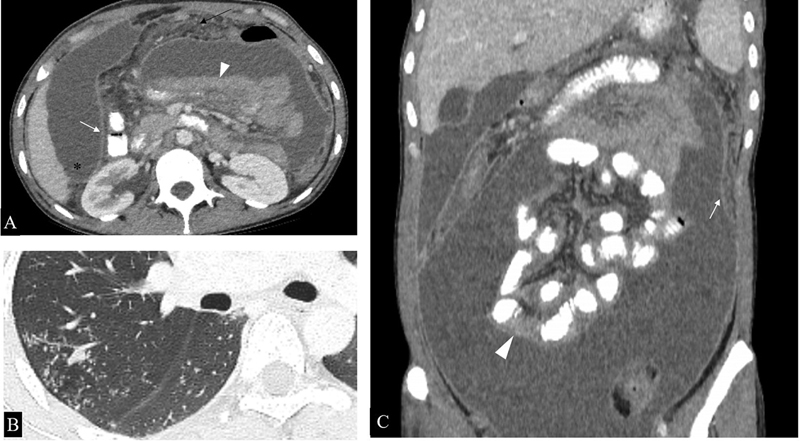
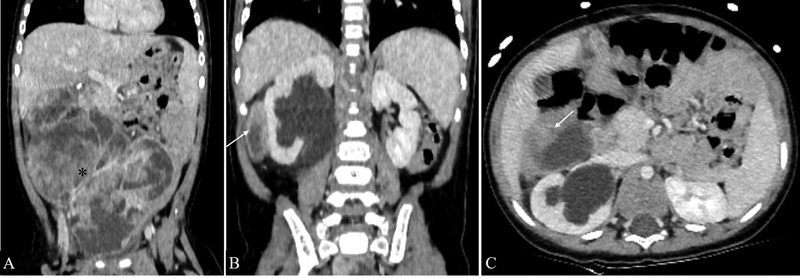
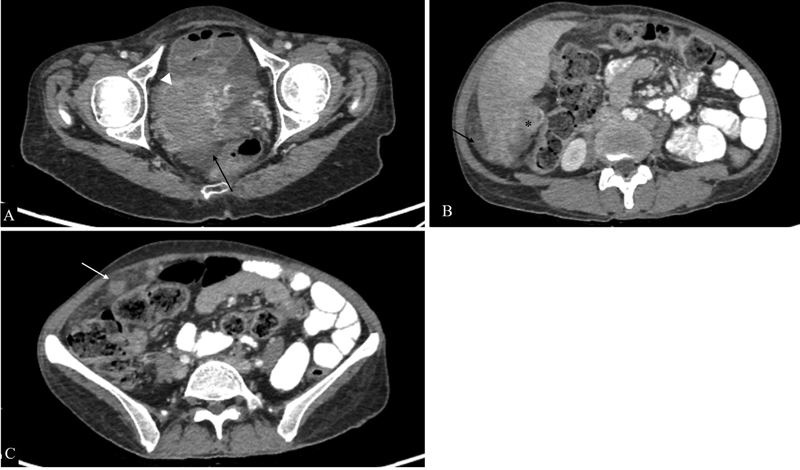
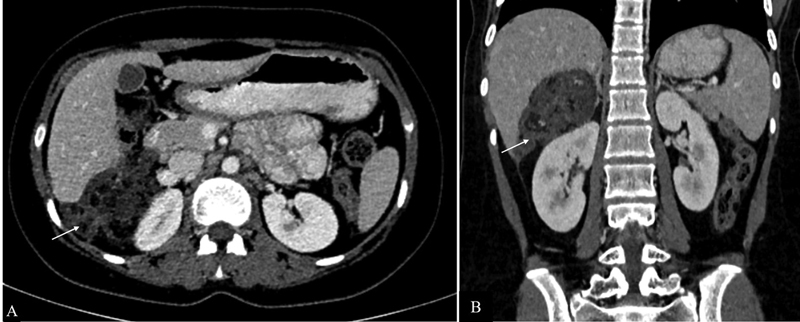
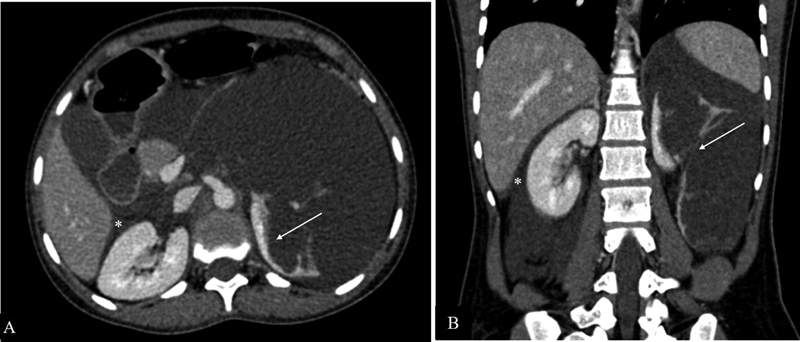
Morrison's pouch is the intraperitoneal space in the supramesocolic compartment located between the right liver lobe and right kidney. Pathological conditions that can involve this peritoneal space include fluid collections, infectious or inflammatory processes, and neoplasms. Frequent involvement by disease entities can be attributed to its dependent location, communication with the inframesocolic compartment, close proximity to the adjacent organs and peritoneal fluid dynamics. Knowledge of the appearance of pathological entities on various imaging modalities helps the radiologist in making the correct diagnosis.
Keywords: CT scan; MRI; Morrison's pouch; peritoneal space.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures



References
-
- Tirkes T, Sandrasegaran K, Patel A A. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics. 2012;32(02):437–451. - PubMed
-
- Meyers M A. Distribution of intra-abdominal malignant seeding: dependency on dynamics of flow of ascitic fluid. Am J Roentgenol Radium Ther Nucl Med. 1973;119(01):198–206. - PubMed
-
- Anthony M P, Khong P L, Zhang J. Spectrum of (18)F-FDG PET/CT appearances in peritoneal disease. AJR Am J Roentgenol. 2009;193(06):W523-9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources