

Blood in the Brain on Susceptibility-Weighted Imaging
- PMID: 36855723
- PMCID: PMC9968548
- DOI: 10.1055/s-0042-1758880
Blood in the Brain on Susceptibility-Weighted Imaging
Abstract
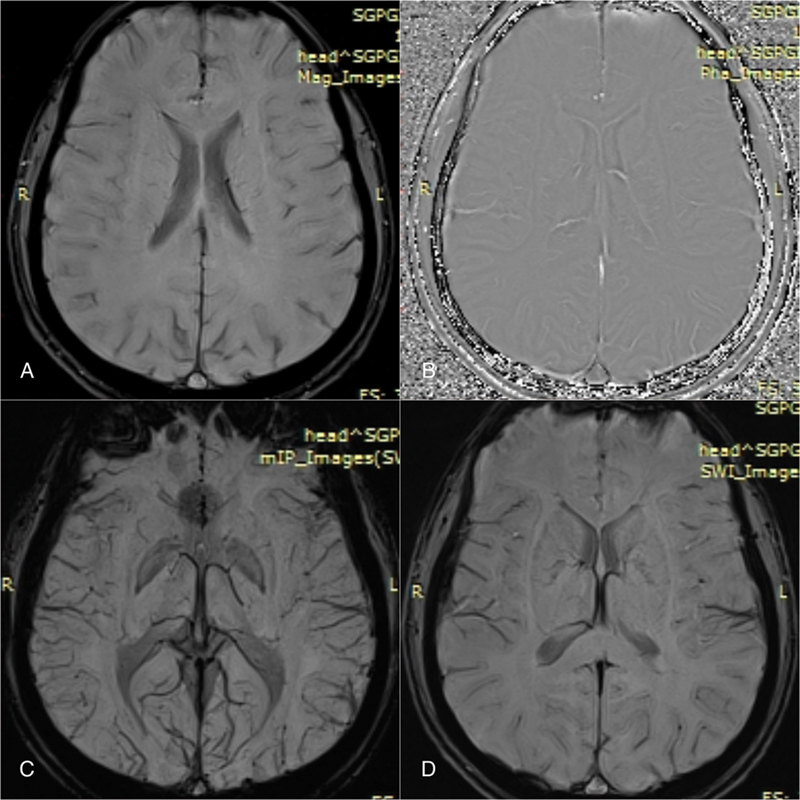
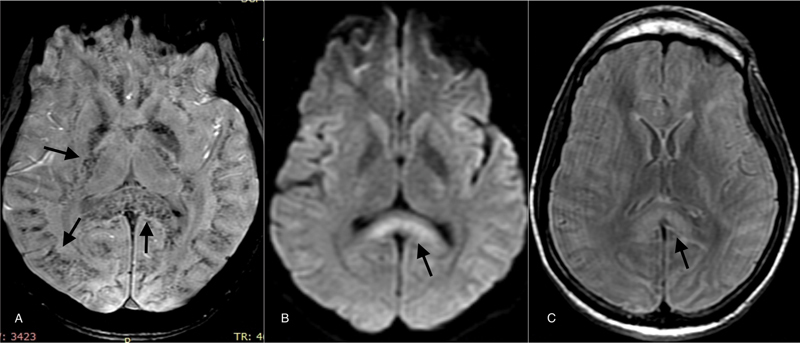
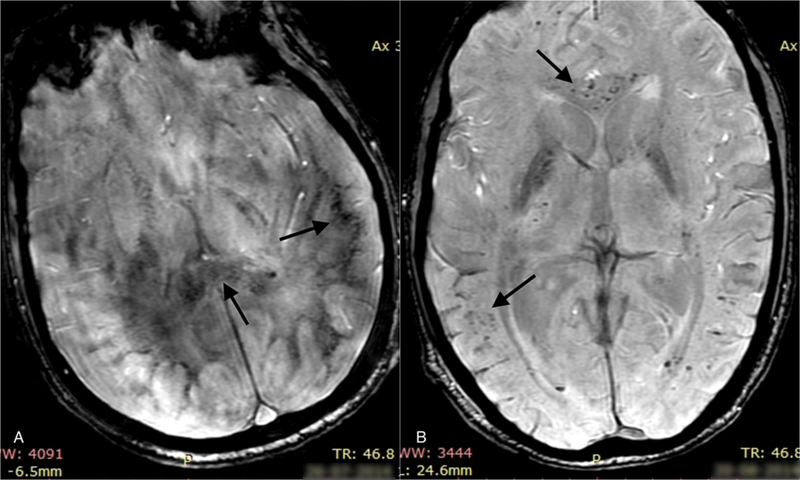
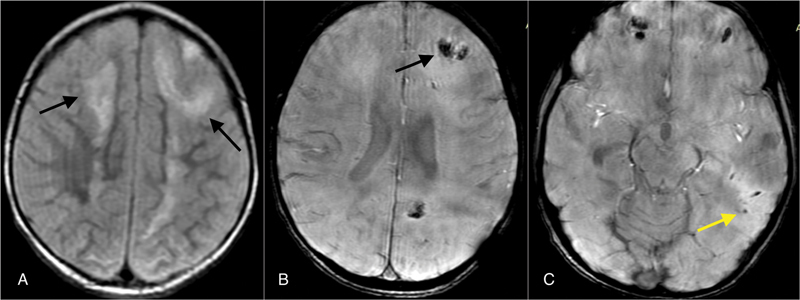
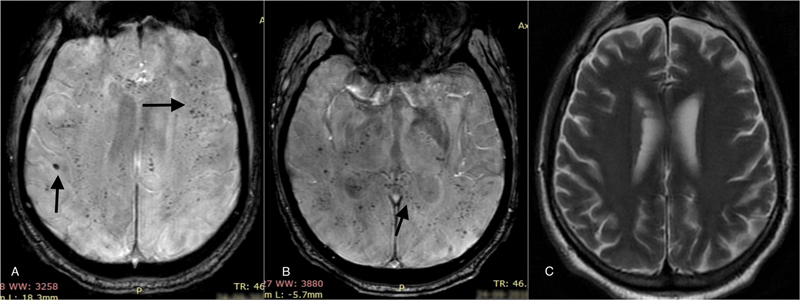
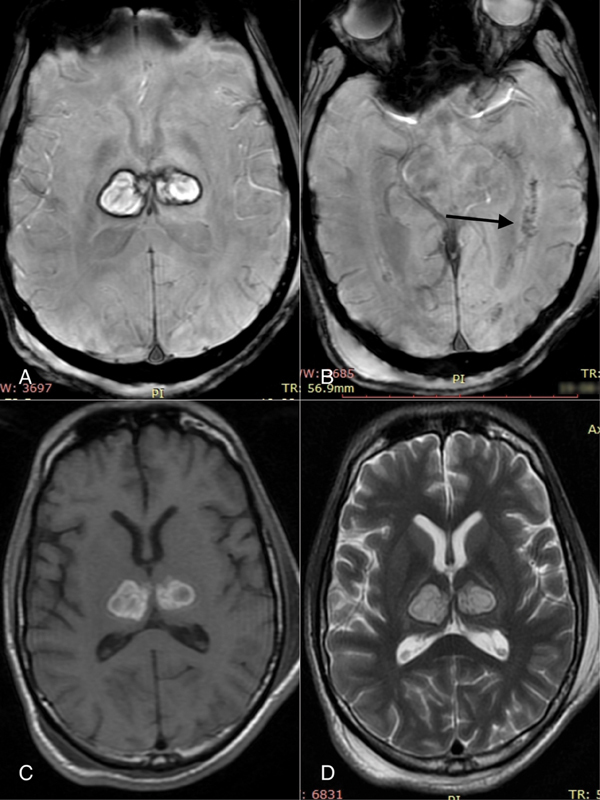
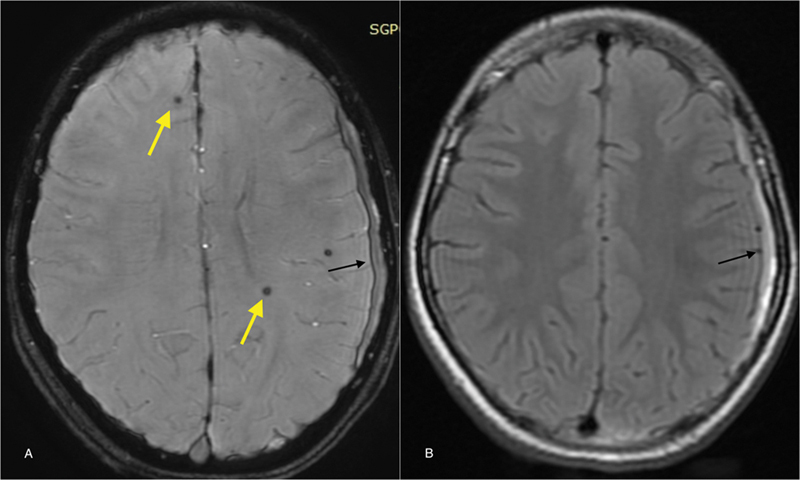
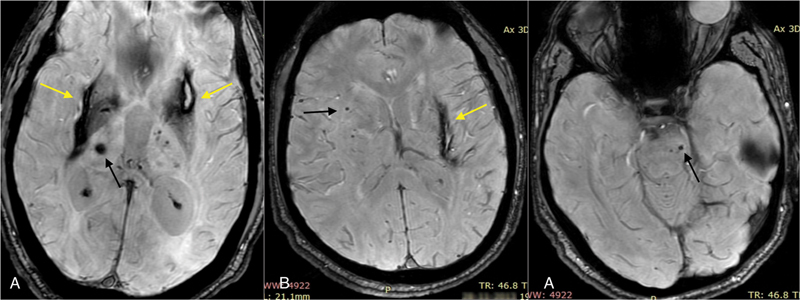
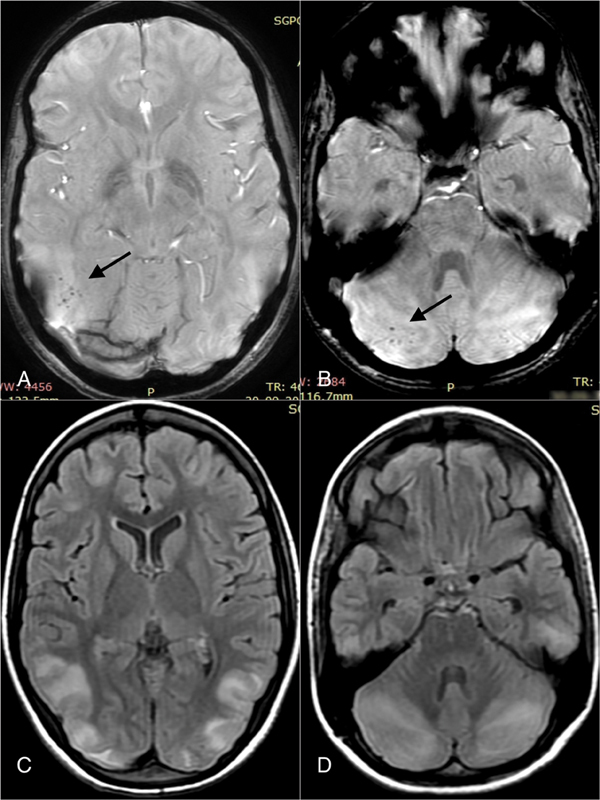
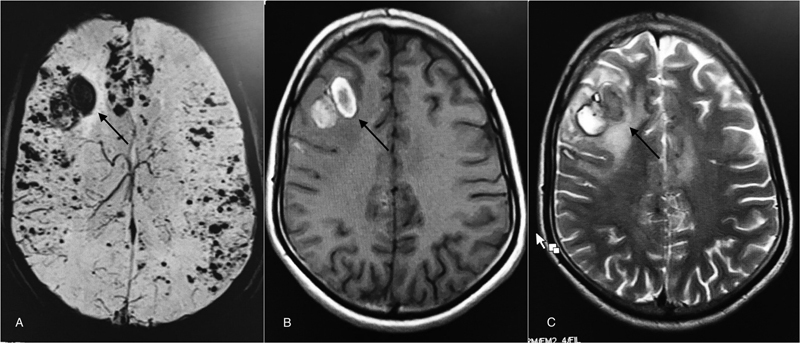
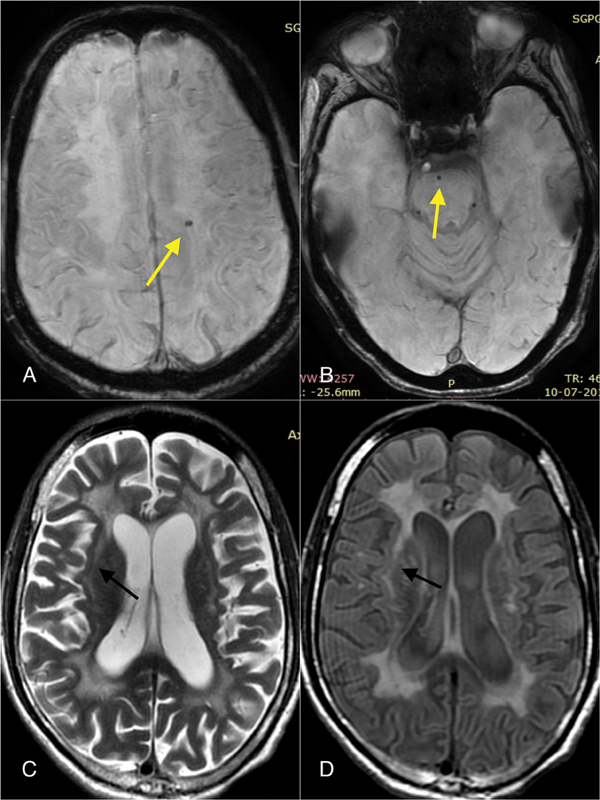
Intraparenchymal brain hemorrhage is not uncommon and results from a wide variety of causes ranging from trauma to tumor. Many a time, it is not possible to determine the exact cause of non-traumatic hemorrhage on conventional magnetic resonance imaging (MRI). Susceptibility-weighted imaging (SWI) is a high-resolution (3D) gradient-echo sequence. It is extremely sensitive to the inhomogeneity of the local magnetic field and highly useful in identifying the small amount of hemorrhage, which may be inapparent on other MR pulse sequences. In this review, we present different pattern of an intra-parenchymal brain hemorrhage on SWI with emphasis on differential diagnosis.
Keywords: brain hemorrhage; hemorrhage; magnetic resonance imaging; microhemorrhage; susceptibility-weighted imaging.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures


Similar articles
-
Susceptibility weighted imaging at 1.5 Tesla magnetic resonance imaging in dogs: Comparison with T2*-weighted gradient echo sequence and its clinical indications.Vet Radiol Ultrasound. 2020 Sep;61(5):566-576. doi: 10.1111/vru.12894. Epub 2020 Jul 14. Vet Radiol Ultrasound. 2020. PMID: 32663373
-
Susceptibility weighted magnetic resonance imaging of brain: A multifaceted powerful sequence that adds to understanding of acute stroke.Ann Indian Acad Neurol. 2014 Jan;17(1):58-61. doi: 10.4103/0972-2327.128555. Ann Indian Acad Neurol. 2014. PMID: 24753661 Free PMC article.
-
Detection of hyperacute primary intraparenchymal hemorrhage by magnetic resonance imaging.Stroke. 1996 Dec;27(12):2321-4. doi: 10.1161/01.str.27.12.2321. Stroke. 1996. PMID: 8969800
-
Susceptibility-weighted imaging and quantitative susceptibility mapping in the brain.J Magn Reson Imaging. 2015 Jul;42(1):23-41. doi: 10.1002/jmri.24768. Epub 2014 Oct 1. J Magn Reson Imaging. 2015. PMID: 25270052 Free PMC article. Review.
-
Susceptibility-Weighted Imaging as a Distinctive Imaging Technique for Providing Complementary Information for Precise Diagnosis of Neurologic Disorder.Taehan Yongsang Uihakhoe Chi. 2021 Jan;82(1):99-115. doi: 10.3348/jksr.2020.0054. Epub 2021 Jan 20. Taehan Yongsang Uihakhoe Chi. 2021. PMID: 36237474 Free PMC article. Review.
Cited by
-
Orthodontic appliances and their diagnostic impact to brain MRI.Clin Oral Investig. 2025 Mar 22;29(4):202. doi: 10.1007/s00784-025-06275-8. Clin Oral Investig. 2025. PMID: 40119988 Free PMC article.
References
-
- Sood S, Gupta R, Modi J, Sharma J.Susceptibility weighted imaging: physics and clinical applications in neuroimaging at 3 Tesla. Conference PaperMarch201410.1594/ecr2014/C-1472 - DOI
-
- Lee Y J, Lee S, Jang J. Findings regarding an intracranial hemorrhage on the phase image of a susceptibility-weighted image (SWI), according to the stage, location, and size. Investig Magn Reson Imaging. 2015;19(02):107–113.
Publication types
LinkOut - more resources
Full Text Sources