

Myocardial Metabolomics of Human Heart Failure With Preserved Ejection Fraction
- PMID: 36856044
- PMCID: PMC11059242
- DOI: 10.1161/CIRCULATIONAHA.122.061846
Myocardial Metabolomics of Human Heart Failure With Preserved Ejection Fraction
Abstract
Background: The human heart primarily metabolizes fatty acids, and this decreases as alternative fuel use rises in heart failure with reduced ejection fraction (HFrEF). Patients with severe obesity and diabetes are thought to have increased myocardial fatty acid metabolism, but whether this is found in those who also have heart failure with preserved ejection fraction (HFpEF) is unknown.
Methods: Plasma and endomyocardial biopsies were obtained from HFpEF (n=38), HFrEF (n=30), and nonfailing donor controls (n=20). Quantitative targeted metabolomics measured organic acids, amino acids, and acylcarnitines in myocardium (72 metabolites) and plasma (69 metabolites). The results were integrated with reported RNA sequencing data. Metabolomics were analyzed using agnostic clustering tools, Kruskal-Wallis test with Dunn test, and machine learning.
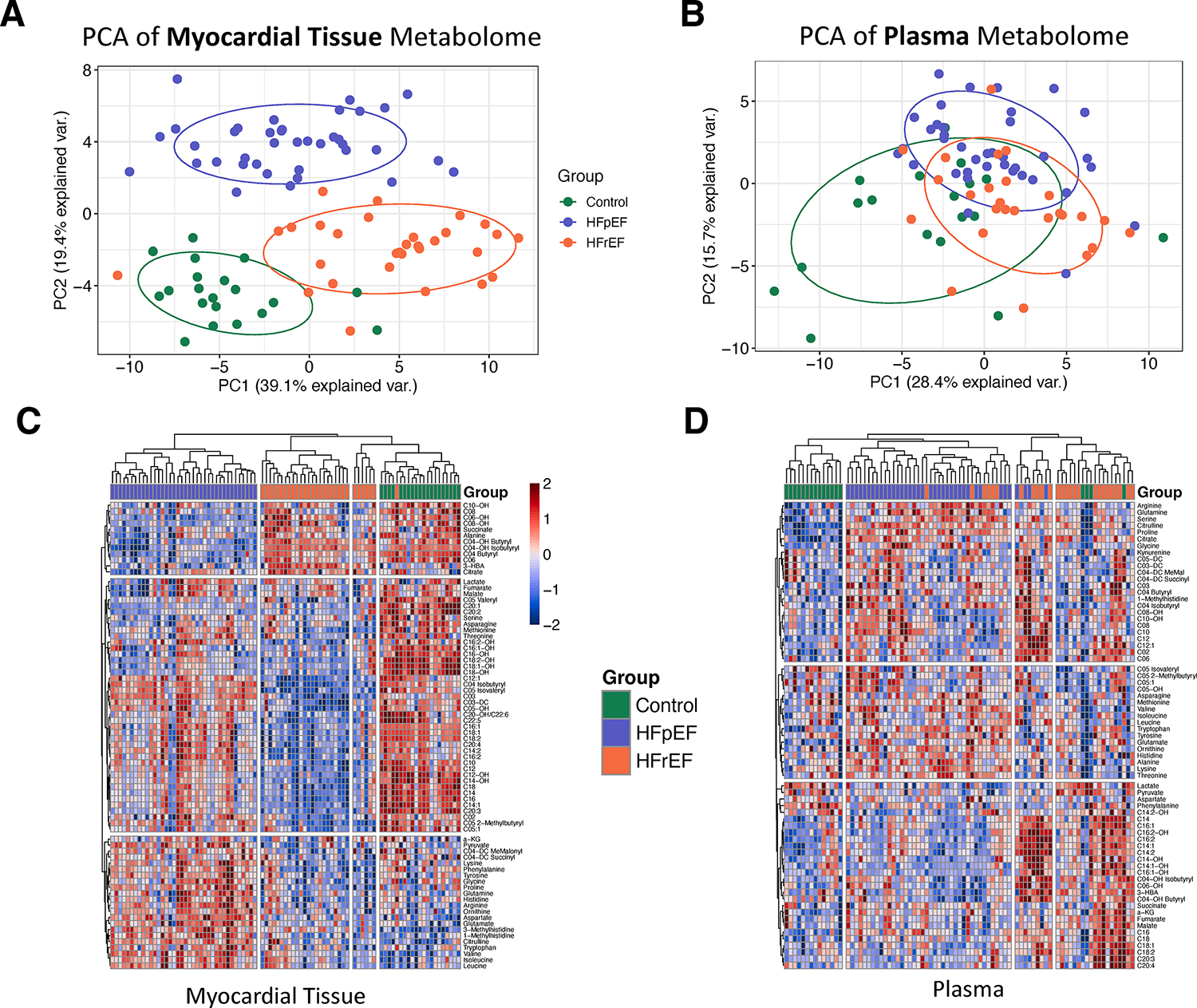
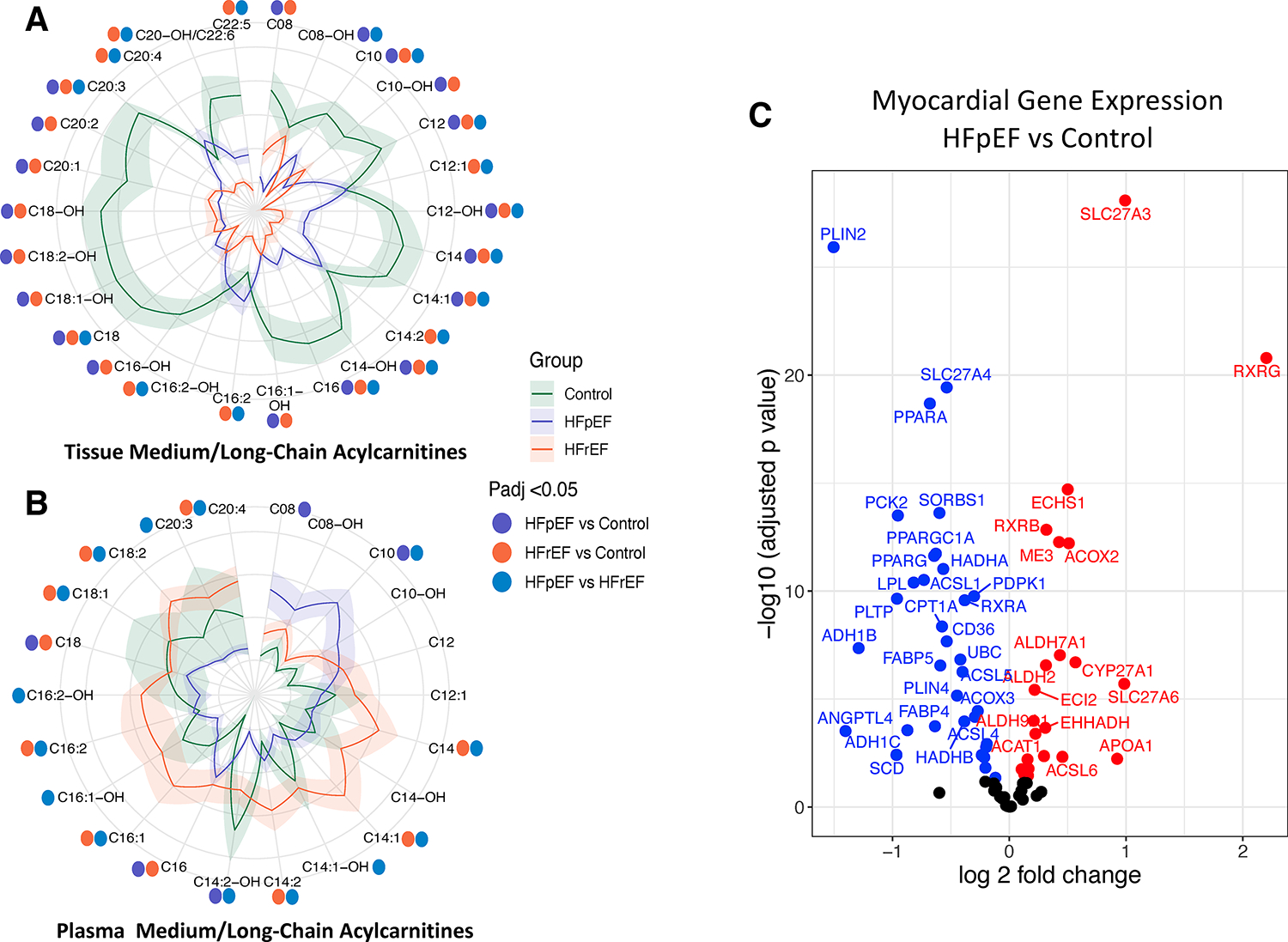
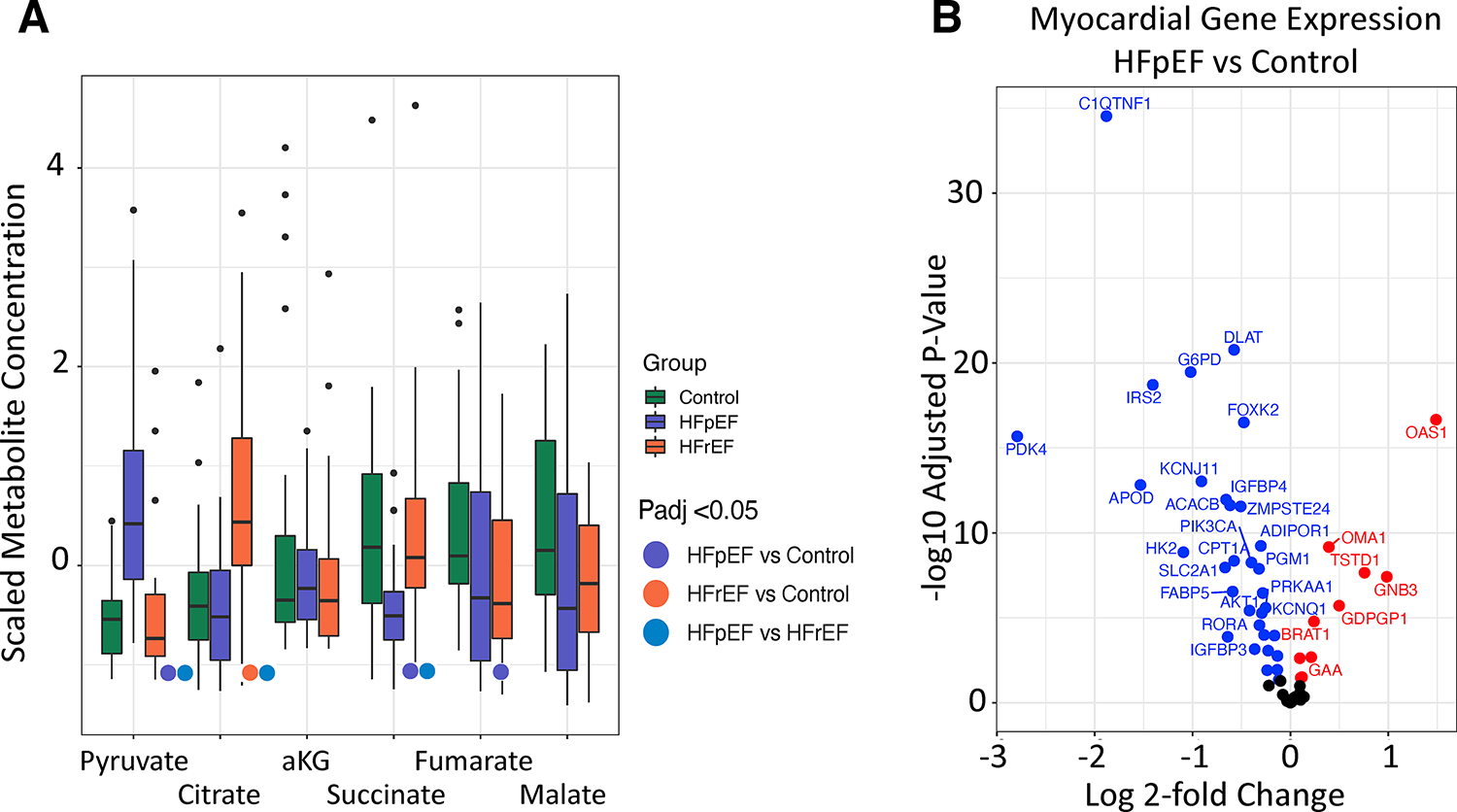
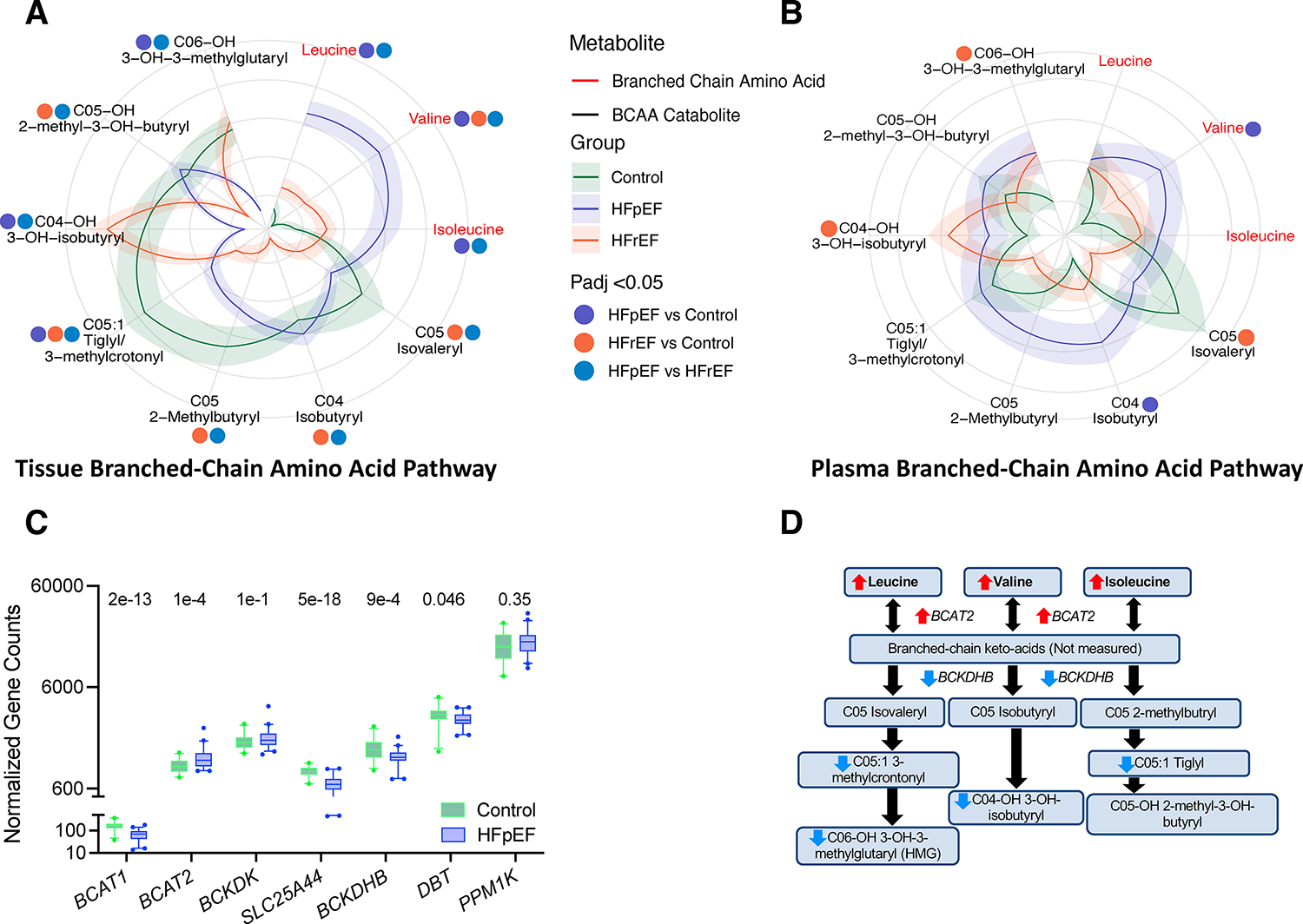
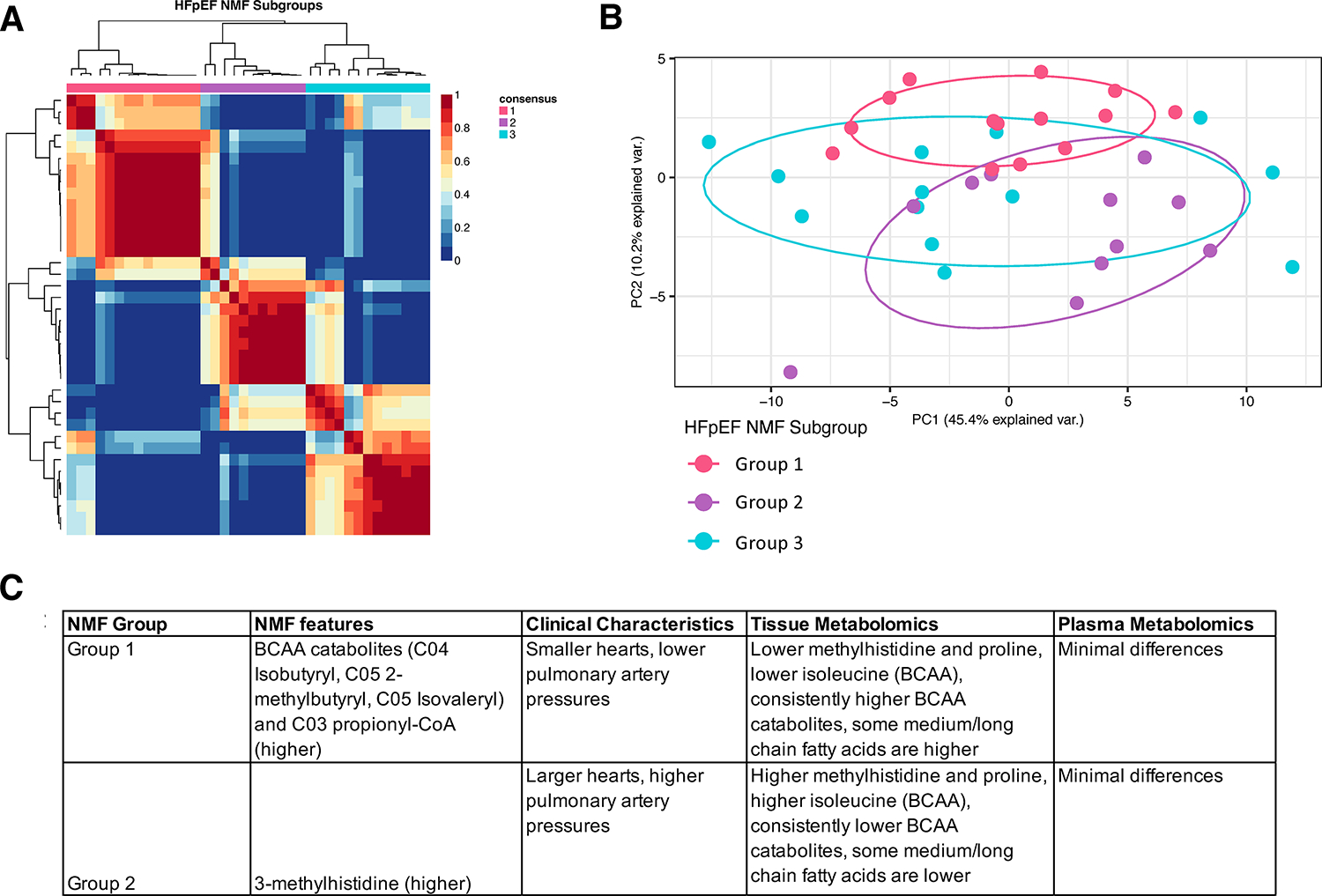
Results: Agnostic clustering of myocardial but not plasma metabolites separated disease groups. Despite more obesity and diabetes in HFpEF versus HFrEF (body mass index, 39.8 kg/m2 versus 26.1 kg/m2; diabetes, 70% versus 30%; both P<0.0001), medium- and long-chain acylcarnitines (mostly metabolites of fatty acid oxidation) were markedly lower in myocardium from both heart failure groups versus control. In contrast, plasma levels were no different or higher than control. Gene expression linked to fatty acid metabolism was generally lower in HFpEF versus control. Myocardial pyruvate was higher in HFpEF whereas the tricarboxylic acid cycle intermediates succinate and fumarate were lower, as were several genes controlling glucose metabolism. Non-branched-chain and branched-chain amino acids (BCAA) were highest in HFpEF myocardium, yet downstream BCAA metabolites and genes controlling BCAA metabolism were lower. Ketone levels were higher in myocardium and plasma of patients with HFrEF but not HFpEF. HFpEF metabolomic-derived subgroups were differentiated by only a few differences in BCAA metabolites.
Conclusions: Despite marked obesity and diabetes, HFpEF myocardium exhibited lower fatty acid metabolites compared with HFrEF. Ketones and metabolites of the tricarboxylic acid cycle and BCAA were also lower in HFpEF, suggesting insufficient use of alternative fuels. These differences were not detectable in plasma and challenge conventional views of myocardial fuel use in HFpEF with marked diabetes and obesity and suggest substantial fuel inflexibility in this syndrome.
Keywords: branched-chain amino acid; heart failure, preserved ejection fraction; human; lipid metabolism; metabolic networks and pathways; metabolomics; obesity.
Conflict of interest statement
Conflict of Interest Disclosures
VS.H, CP, MSK, KCB, HW, SM, NK, EJY, ZA- none. KBM receives research grant funding from Amgen, Inc. and serves on an advisory board for Bristol-Myers-Squibb. DPK serves on the advisory boards for Pfizer and Amgen, and receives grant funding from Amgen. DAK serves on advisory boards for Amgen, Cytokinetics, Cardurion, Boehringer-Ingelheim, and AstraZeneca. He also receives grant funding from Cytokinetics, Amgen, and Boehringer-Ingelheim. KS serves as an advisory board member and/or consultant to AstraZeneca, Alleviant, Bayer, Boehringer-Ingelheim, Imbria, Novartis, NovoNordisk, RIVUS, and ViCardia. She receives grant support from Amgen.
Figures
References
-
- Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC and Coats A. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc Res. 2023; 118(17):3272–3287. - PubMed
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, Elkind MSV, Evenson KR, Ferguson JF, Gupta DK, Khan SS, Kissela BM, Knutson KL, Lee CD, Lewis TT, Liu J, Loop MS, Lutsey PL, Ma J, Mackey J, Martin SS, Matchar DB, Mussolino ME, Navaneethan SD, Perak AM, Roth GA, Samad Z, Satou GM, Schroeder EB, Shah SH, Shay CM, Stokes A, VanWagner LB, Wang NY, Tsao CW, American Heart Association Council on E, Prevention Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation. 2021;143:e254–e743. - PubMed
-
- Runte KE, Bell SP, Selby DE, Häußler TN, Ashikaga T, LeWinter MM, Palmer BM and Meyer M. Relaxation and the Role of Calcium in Isolated Contracting Myocardium From Patients With Hypertensive Heart Disease and Heart Failure With Preserved Ejection Fraction. Circ Heart Fail. 2017;10:e004311. - PMC - PubMed
-
- van Heerebeek L, Hamdani N, Falcao-Pires I, Leite-Moreira AF, Begieneman MP, Bronzwaer JG, van der Velden J, Stienen GJ, Laarman GJ, Somsen A, Verheugt FW, Niessen HW and Paulus WJ. Low myocardial protein kinase G activity in heart failure with preserved ejection fraction. Circulation. 2012;126:830–9. - PubMed
-
- Westermann D, Lindner D, Kasner M, Zietsch C, Savvatis K, Escher F, von Schlippenbach J, Skurk C, Steendijk P, Riad A, Poller W, Schultheiss HP and Tschope C. Cardiac inflammation contributes to changes in the extracellular matrix in patients with heart failure and normal ejection fraction. Circ Heart Fail. 2011;4:44–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL128349/HL/NHLBI NIH HHS/United States
- K23 HL166770/HL/NHLBI NIH HHS/United States
- R01 HL149891/HL/NHLBI NIH HHS/United States
- R01 HL133080/HL/NHLBI NIH HHS/United States
- P30 DK050306/DK/NIDDK NIH HHS/United States
- L30 HL138884/HL/NHLBI NIH HHS/United States
- T32 HL007227/HL/NHLBI NIH HHS/United States
- R01 HL061912/HL/NHLBI NIH HHS/United States
- R01 HL105993/HL/NHLBI NIH HHS/United States
- R01 HL151345/HL/NHLBI NIH HHS/United States
- R01 HL152446/HL/NHLBI NIH HHS/United States
- R35 HL135827/HL/NHLBI NIH HHS/United States
- P30 CA016520/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
