

Non-Rheumatic Chronic Comorbidities in Children with Juvenile Idiopathic Arthritis
- PMID: 36856360
- PMCID: PMC10081080
- DOI: 10.5152/TurkArchPediatr.2023.22303
Non-Rheumatic Chronic Comorbidities in Children with Juvenile Idiopathic Arthritis
Abstract
Objective: Juvenile idiopathic arthritis is a heterogeneous group of disorders and is the most common rheumatic condition in childhood. There are scarce data regarding all comorbidities in juvenile idiopathic arthritis patients.
Materials and methods: We aimed to identify the non-rheumatic comorbidities in our juvenile idiopathic arthritis patients. Data were obtained cross-sectionally from the medical records and the face-to-face interviews for 6 consecutive months. Those with more than 1 rheumatic disease were excluded, and conditions that were highly related to the disease, such as uveitis, were not taken into account.
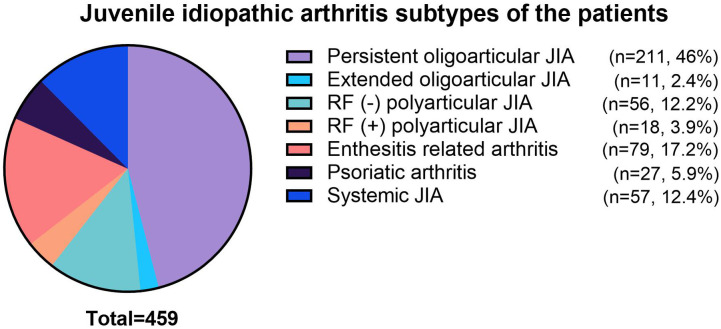
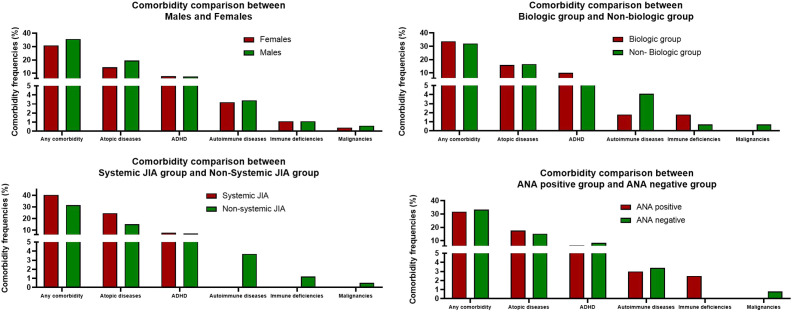
Results: The study included 459 patients with female dominance (62.1%, n = 285). The median age of the patients was 12.87 (1.53-20.95) years. One hundred fifty patients (32.7%) had at least 1 comorbidity (5 patients had 3 comorbidities, and 24 patients had 2 comorbidities). The most common 3 non-rheumatic accompanying medical conditions in our patients were allergic rhinitis (n = 37, 8.1%), attention-deficit hyperactivity disorder (n = 35, 7.6%), and atopic dermatitis (n = 28, 6.1%). None of our patients with systemic JIA had any autoimmune disease. All the patients with primary immune deficiencies had anti-nuclear antibody positivity.
Conclusion: Almost one-third of our patients had at least one comorbidity. This finding might be very helpful to us in planning our multi-disciplinary approach to our patients.
Figures
References
LinkOut - more resources
Full Text Sources