

Outcome in Children Admitted to the First PICU in Malawi
- PMID: 36856446
- PMCID: PMC10226467
- DOI: 10.1097/PCC.0000000000003210
Outcome in Children Admitted to the First PICU in Malawi
Abstract
Objectives: Dedicated PICUs are slowly starting to emerge in sub-Saharan Africa. Establishing these units can be challenging as there is little data from this region to inform which populations and approaches should be prioritized. This study describes the characteristics and outcome of patients admitted to the first PICU in Malawi, with the aim to identify factors associated with increased mortality.
Design: Review of a prospectively constructed PICU database. Univariate analysis was used to assess associations between demographic, clinical and laboratory factors, and mortality. Univariate associations ( p < 0.1) for mortality were entered in two multivariable models.
Setting: A recently opened PICU in a public tertiary government hospital in Blantyre, Malawi.
Patients: Children admitted to PICU between August 1, 2017, and July 31, 2019.
Interventions: None.
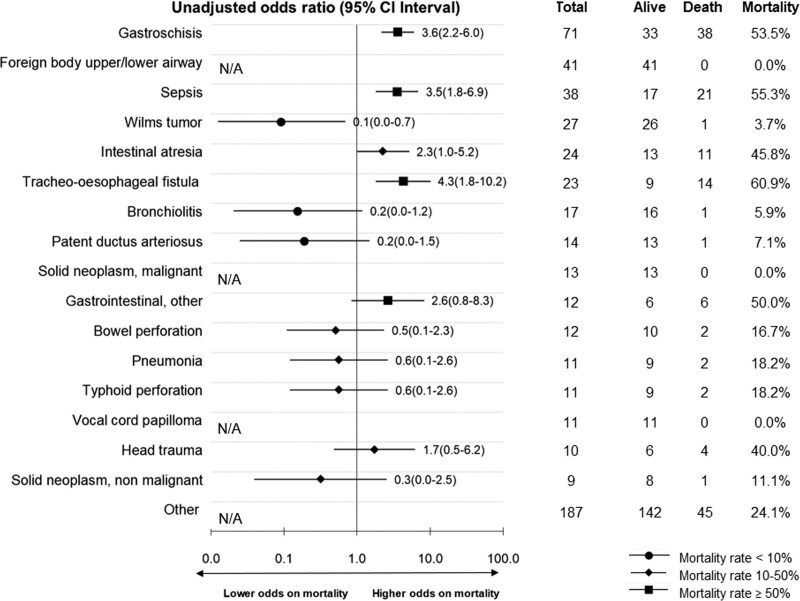
Measurement and main results: Of 531 included PICU admissions, 149 children died (28.1%). Mortality was higher in neonates (88/167; 52.7%) than older children (61/364; 16.8%; p ≤ 0.001). On univariate analysis, gastroschisis, trachea-esophageal fistula, and sepsis had higher PICU mortality, while Wilms tumor, other neoplasms, vocal cord papilloma, and foreign body aspiration had higher survival rates compared with other conditions. On multivariable analysis, neonatal age (adjusted odds ratio [AOR], 4.0; 95% CI, 2.0-8.3), decreased mental state (AOR, 5.8; 95 CI, 2.4-13.8), post-cardiac arrest (AOR, 2.0; 95% CI, 1.0-8.0), severe hypotension (AOR, 6.3; 95% CI, 2.0-19.1), lactate greater than 5 mmol/L (AOR, 4.2; 95% CI, 1.5-11.2), pH less than 7.2 (AOR, 3.1; 95% CI, 1.2-8.0), and platelets less than 150 × 10 9 /L (AOR, 2.4; 95% CI, 1.1-5.2) were associated with increased mortality.
Conclusions: In the first PICU in Malawi, mortality was relatively high, especially in neonates. Surgical neonates and septic patients were identified as highly vulnerable, which stresses the importance of improvement of PICU care bundles for these groups. Several clinical and laboratory variables were associated with mortality in older children. In neonates, severe hypotension was the only clinical variable associated with increased mortality besides blood gas parameters. This stresses the importance of basic laboratory tests, especially in neonates. These data contribute to evidence-based approaches establishing and improving future PICUs in sub-Saharan Africa.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Drs. de Visser and Calis received support for article research from the Mercy James Center which is primarily supported by the Paediatric Surgical Trust and the Government of Malawi’s Ministry of Health. Dr. Bentsen disclosed government work. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Pediatric Intensive Care Development When Resources Are Scarce and Demand Is Potentially Very High.Pediatr Crit Care Med. 2023 Jun 1;24(6):525-527. doi: 10.1097/PCC.0000000000003260. Epub 2023 Jun 1. Pediatr Crit Care Med. 2023. PMID: 37260338 No abstract available.
References
-
- World Health Organization: Children: Improving Survival and Well-Being. 2020. Available at: https://www.who.int/news-room/fact-sheets/detail/children-reducing-morta.... Accessed January 10, 2021
-
- Kissoon N, Burns J: Who should get pediatric intensive care when not all can? A call for international guidelines on allocation of pediatric intensive care resources. Pediatr Crit Care Med. 2014; 15:82–83 - PubMed
-
- Calis JC, Weir P, Kapalamula T, et al. : Establishing a paediatric intensive care unit in a low income setting. MTb- Bull Netherlands Soc Trop Med Int Heal. 2019; 57:6–9
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
