

Neoadjuvant-Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma
- PMID: 36856617
- PMCID: PMC10410527
- DOI: 10.1056/NEJMoa2211437
Neoadjuvant-Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma
Abstract
Background: Whether pembrolizumab given both before surgery (neoadjuvant therapy) and after surgery (adjuvant therapy), as compared with pembrolizumab given as adjuvant therapy alone, would increase event-free survival among patients with resectable stage III or IV melanoma is unknown.
Methods: In a phase 2 trial, we randomly assigned patients with clinically detectable, measurable stage IIIB to IVC melanoma that was amenable to surgical resection to three doses of neoadjuvant pembrolizumab, surgery, and 15 doses of adjuvant pembrolizumab (neoadjuvant-adjuvant group) or to surgery followed by pembrolizumab (200 mg intravenously every 3 weeks for a total of 18 doses) for approximately 1 year or until disease recurred or unacceptable toxic effects developed (adjuvant-only group). The primary end point was event-free survival in the intention-to-treat population. Events were defined as disease progression or toxic effects that precluded surgery; the inability to resect all gross disease; disease progression, surgical complications, or toxic effects of treatment that precluded the initiation of adjuvant therapy within 84 days after surgery; recurrence of melanoma after surgery; or death from any cause. Safety was also evaluated.
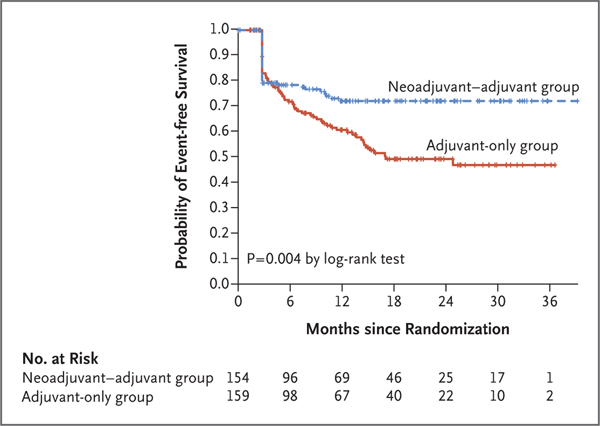
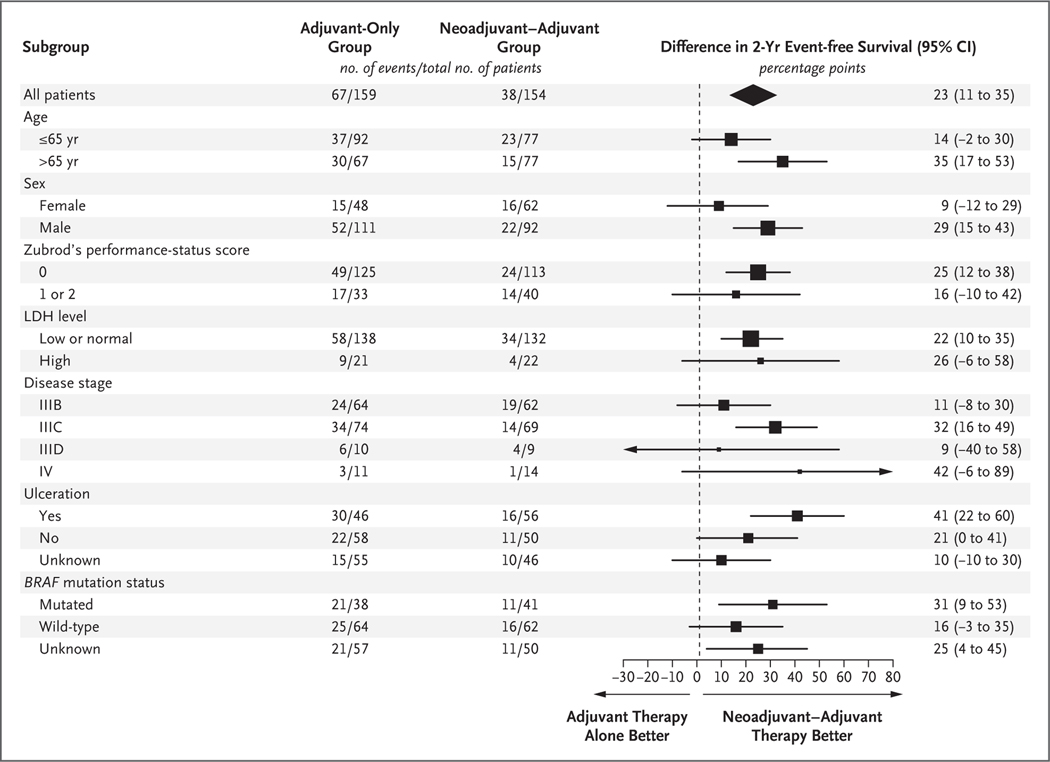
Results: At a median follow-up of 14.7 months, the neoadjuvant-adjuvant group (154 patients) had significantly longer event-free survival than the adjuvant-only group (159 patients) (P = 0.004 by the log-rank test). In a landmark analysis, event-free survival at 2 years was 72% (95% confidence interval [CI], 64 to 80) in the neoadjuvant-adjuvant group and 49% (95% CI, 41 to 59) in the adjuvant-only group. The percentage of patients with treatment-related adverse events of grades 3 or higher during therapy was 12% in the neoadjuvant-adjuvant group and 14% in the adjuvant-only group.
Conclusions: Among patients with resectable stage III or IV melanoma, event-free survival was significantly longer among those who received pembrolizumab both before and after surgery than among those who received adjuvant pembrolizumab alone. No new toxic effects were identified. (Funded by the National Cancer Institute and Merck Sharp and Dohme; S1801 ClinicalTrials.gov number, NCT03698019.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Neoadjuvant pembrolizumab improves outcomes.Nat Rev Clin Oncol. 2023 May;20(5):284. doi: 10.1038/s41571-023-00752-3. Nat Rev Clin Oncol. 2023. PMID: 36899061 No abstract available.
-
Neoadjuvant immunotherapy improves outlook in high-risk melanoma.Cancer. 2023 Jul 1;129(13):1952. doi: 10.1002/cncr.34884. Cancer. 2023. PMID: 37300812 No abstract available.
References
-
- Weber J, Mandala M, Del Vecchio M, et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N Engl J Med 2017; 377: 1824–35. - PubMed
-
- Eggermont AMM, Blank CU, Mandala M, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med 2018; 378: 1789–801. - PubMed
-
- Sharma P, Allison JP. The future of immune checkpoint therapy. Science 2015; 348:5 6–61. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UG1 CA233331/CA/NCI NIH HHS/United States
- UG1 CA233320/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- UG1CA189860/CA/NCI NIH HHS/United States
- UG1 CA233193/CA/NCI NIH HHS/United States
- UG1CA189869/CA/NCI NIH HHS/United States
- UG1CA239767/CA/NCI NIH HHS/United States
- UG1 CA233247/CA/NCI NIH HHS/United States
- U10CA180819/CA/NCI NIH HHS/United States
- UG1CA233320/CA/NCI NIH HHS/United States
- U10 CA180868/CA/NCI NIH HHS/United States
- U10CA180888/CA/NCI NIH HHS/United States
- UG1CA189956/CA/NCI NIH HHS/United States
- UG1 CA233329/CA/NCI NIH HHS/United States
- UG1 CA189821/CA/NCI NIH HHS/United States
- UG1CA189830/CA/NCI NIH HHS/United States
- P30CA014089/CA/NCI NIH HHS/United States
- UG1CA189850/CA/NCI NIH HHS/United States
- UG1 CA233178/CA/NCI NIH HHS/United States
- UG1CA233328/CA/NCI NIH HHS/United States
- UG1CA233160/CA/NCI NIH HHS/United States
- UG1 CA233234/CA/NCI NIH HHS/United States
- P30CA033572/CA/NCI NIH HHS/United States
- U10CA180821/CA/NCI NIH HHS/United States
- UG1CA239758/CA/NCI NIH HHS/United States
- UG1 CA233330/CA/NCI NIH HHS/United States
- UG1 CA189869/CA/NCI NIH HHS/United States
- UG1 CA189956/CA/NCI NIH HHS/United States
- UG1CA233329/CA/NCI NIH HHS/United States
- UG1CA180830/CA/NCI NIH HHS/United States
- U10CA180820/CA/NCI NIH HHS/United States
- R35 CA197633/CA/NCI NIH HHS/United States
- P50 CA121973/CA/NCI NIH HHS/United States
- UG1 CA180830/CA/NCI NIH HHS/United States
- UG1 CA189860/CA/NCI NIH HHS/United States
- P30CA076292/CA/NCI NIH HHS/United States
- UG1CA233178/CA/NCI NIH HHS/United States
- P30 CA076292/CA/NCI NIH HHS/United States
- P30 CA016042/CA/NCI NIH HHS/United States
- UG1 CA233160/CA/NCI NIH HHS/United States
- U10CA180868/CA/NCI NIH HHS/United States
- P30 CA014089/CA/NCI NIH HHS/United States
- UG1CA233180/CA/NCI NIH HHS/United States
- UG1 CA189850/CA/NCI NIH HHS/United States
- UG1 CA189830/CA/NCI NIH HHS/United States
- UG1 CA239767/CA/NCI NIH HHS/United States
- UG1CA233234/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- UG1CA233247/CA/NCI NIH HHS/United States
- P01 CA244118/CA/NCI NIH HHS/United States
- UG1CA233193/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- P30 CA033572/CA/NCI NIH HHS/United States
- UG1CA189821/CA/NCI NIH HHS/United States
- P30CA016042/CA/NCI NIH HHS/United States
- UG1 CA239758/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- UG1 CA233184/CA/NCI NIH HHS/United States
- U10 CA180819/CA/NCI NIH HHS/United States
- UG1CA233330/CA/NCI NIH HHS/United States
- UG1 CA233328/CA/NCI NIH HHS/United States
- UG1CA233331/CA/NCI NIH HHS/United States