

Diagnostic Accuracy of Epilepsy-dedicated MRI with Post-processing
- PMID: 36856785
- PMCID: PMC10449992
- DOI: 10.1007/s00062-023-01265-3
Diagnostic Accuracy of Epilepsy-dedicated MRI with Post-processing
Abstract
Purpose: To evaluate the diagnostic accuracy of epilepsy-dedicated 3 Tesla MRI including post-processing by correlating MRI, histopathology, and postsurgical seizure outcomes.
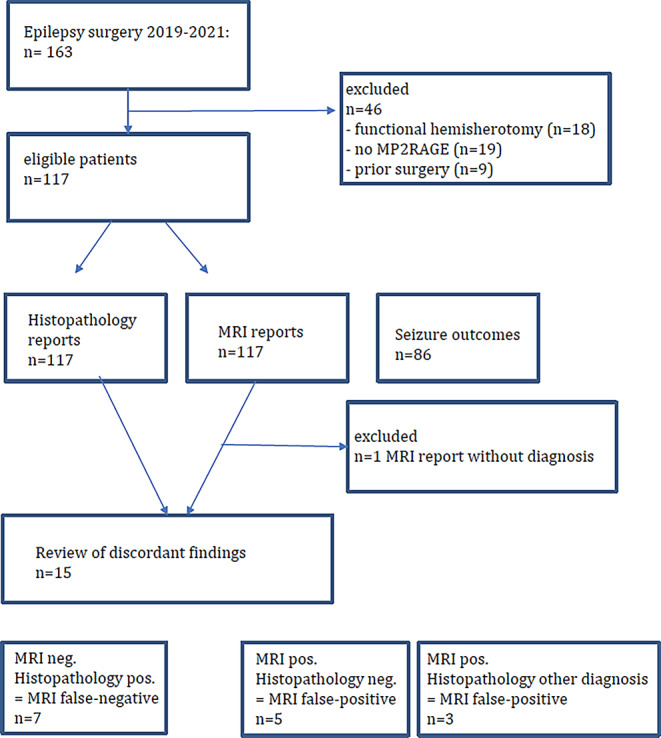
Methods: 3 Tesla-MRI including a magnetization-prepared two rapid acquisition gradient echo (MP2RAGE) sequence for post-processing using the morphometric analysis program MAP was acquired in 116 consecutive patients with drug-resistant focal epilepsy undergoing resection surgery. The MRI, histopathology reports and postsurgical seizure outcomes were recorded from the patient's charts.
Results: The MRI and histopathology were concordant in 101 and discordant in 15 patients, 3 no hippocampal sclerosis/gliosis only lesions were missed on MRI and 1 of 28 focal cortical dysplasia (FCD) type II associated with a glial scar was considered a glial scar only on MRI. In another five patients, MRI was suggestive of FCD, the histopathology was uneventful but patients were seizure-free following surgery. The MRI and histopathology were concordant in 20 of 21 glioneuronal tumors, 6 cavernomas, and 7 glial scars. Histopathology was negative in 10 patients with temporal lobe epilepsy, 4 of them had anteroinferior meningoencephaloceles. Engel class IA outcome was reached in 71% of patients.
Conclusion: The proposed MRI protocol is highly accurate. No hippocampal sclerosis/gliosis only lesions are typically MRI negative. Small MRI positive FCD can be histopathologically missed, most likely due to sampling errors resulting from insufficient harvesting of tissue.
Keywords: Epilepsy; Lesion; MP2RAGE; MRI; Post-processing.
© 2023. The Author(s).
Conflict of interest statement
H. Urbach, C. Scheiwe, M.J. Shah, J.M. Nakagawa, M. Heers, M.V. San Antonio-Arce, D.-M. Altenmueller, A. Schulze-Bonhage, H.-J. Huppertz, T. Demerath and S. Doostkam declare that they have no competing interests.
Figures




References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
