

Risk for stillbirth among pregnant individuals with SARS-CoV-2 infection varied by gestational age
- PMID: 36858096
- PMCID: PMC9970919
- DOI: 10.1016/j.ajog.2023.02.022
Risk for stillbirth among pregnant individuals with SARS-CoV-2 infection varied by gestational age
Abstract
Background: Despite previous research findings on higher risks of stillbirth among pregnant individuals with SARS-CoV-2 infection, it is unclear whether the gestational timing of viral infection modulates this risk.
Objective: This study aimed to examine the association between timing of SARS-CoV-2 infection during pregnancy and risk of stillbirth.
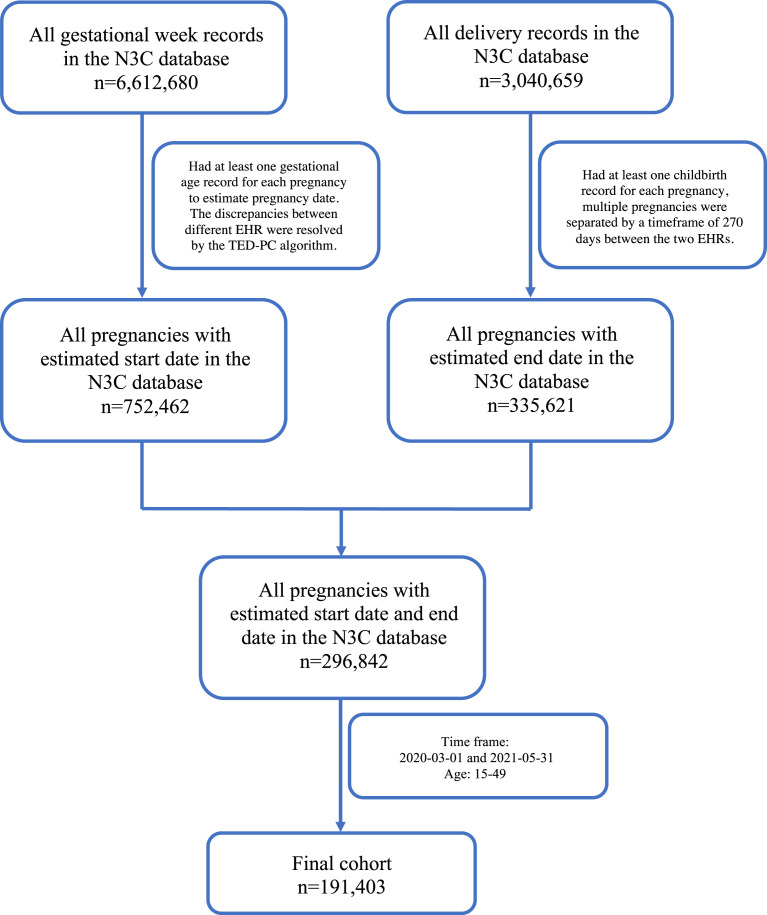
Study design: This retrospective cohort study used multilevel logistic regression analyses of nationwide electronic health records in the United States. Data were from 75 healthcare systems and institutes across 50 states. A total of 191,403 pregnancies of 190,738 individuals of reproductive age (15-49 years) who had childbirth between March 1, 2020 and May 31, 2021 were identified and included. The main outcome was stillbirth at ≥20 weeks of gestation. Exposures were the timing of SARS-CoV-2 infection: early pregnancy (<20 weeks), midpregnancy (21-27 weeks), the third trimester (28-43 weeks), any time before delivery, and never infected (reference).
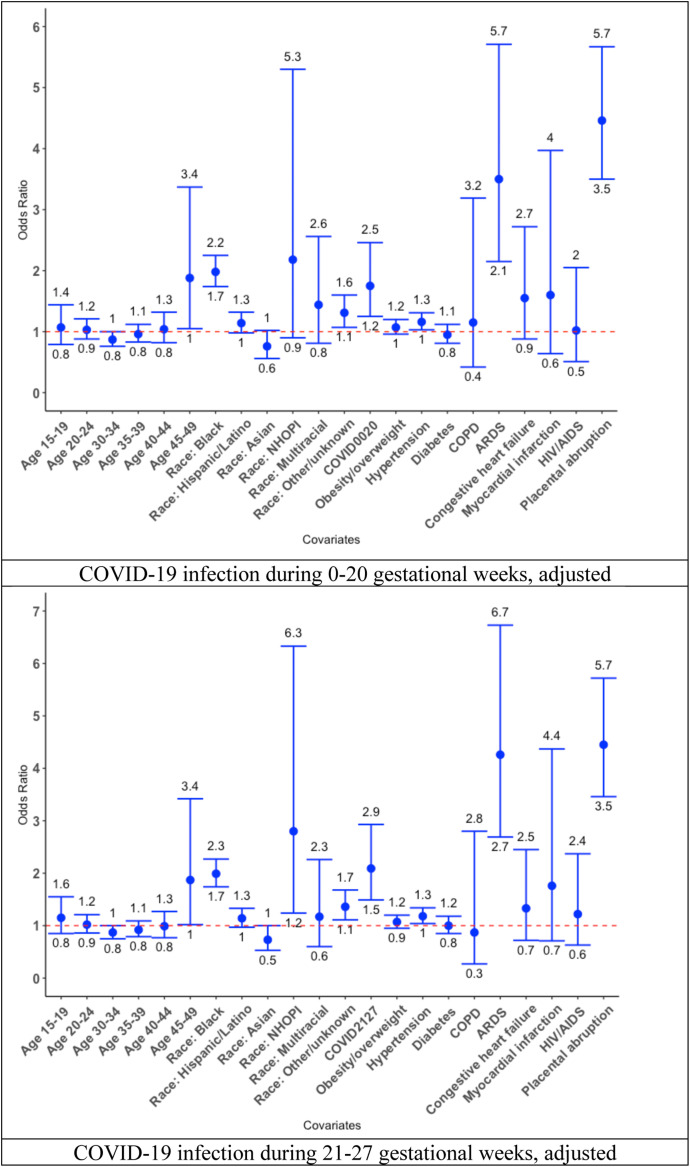
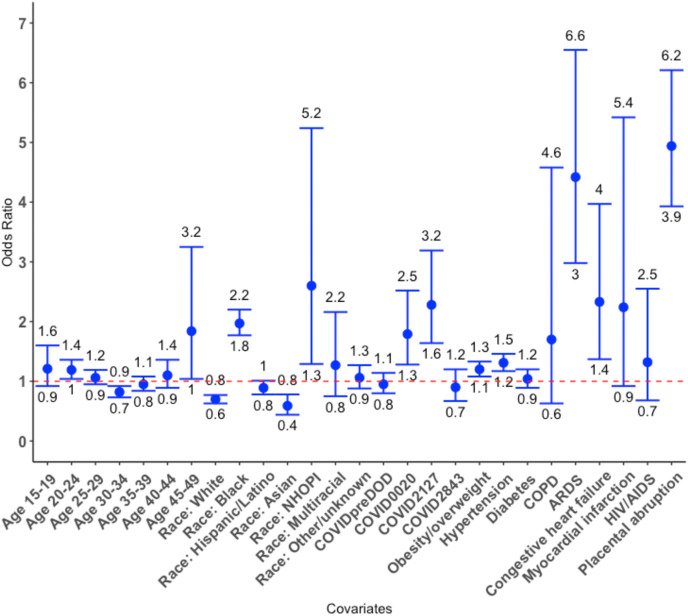
Results: We identified 2342 (1.3%) pregnancies with COVID-19 in early pregnancy, 2075 (1.2%) in midpregnancy, and 12,697 (6.9%) in the third trimester. After adjusting for maternal and clinical characteristics, increased odds of stillbirth were observed among pregnant individuals with SARS-CoV-2 infection only in early pregnancy (odds ratio, 1.75, 95% confidence interval, 1.25-2.46) and midpregnancy (odds ratio, 2.09; 95% confidence interval, 1.49-2.93), as opposed to pregnant individuals who were never infected. Older age, Black race, hypertension, acute respiratory distress syndrome or acute respiratory failure, and placental abruption were found to be consistently associated with stillbirth across different trimesters.
Conclusion: Increased risk of stillbirth was associated with COVID-19 only when pregnant individuals were infected during early and midpregnancy, and not at any time before the delivery or during the third trimester, suggesting the potential vulnerability of the fetus to SARS-CoV-2 infection in early pregnancy. Our findings underscore the importance of proactive COVID-19 prevention and timely medical intervention for individuals infected with SARS-CoV-2 during early and midpregnancy.
Keywords: COVID-19; electronic health records; gynecology; obstetrics; pregnancy; stillbirth.
Copyright © 2023 Elsevier Inc. All rights reserved.
Figures
References
-
- The New York Times Coronavirus in the U.S.: latest map and case count. 2022. https://www.nytimes.com/interactive/2021/us/covid-cases.html Available at:
Publication types
MeSH terms
Grants and funding
- UM1 TR004404/TR/NCATS NIH HHS/United States
- UL1 TR002649/TR/NCATS NIH HHS/United States
- UL1 TR001433/TR/NCATS NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- UL1 TR001860/TR/NCATS NIH HHS/United States
- UL1 TR001427/TR/NCATS NIH HHS/United States
- U54 GM104942/GM/NIGMS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1 TR001439/TR/NCATS NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- UL1 TR001445/TR/NCATS NIH HHS/United States
- UL1 TR003096/TR/NCATS NIH HHS/United States
- U54 GM104938/GM/NIGMS NIH HHS/United States
- R01 AI127203/AI/NIAID NIH HHS/United States
- UL1 TR002537/TR/NCATS NIH HHS/United States
- UL1 TR001412/TR/NCATS NIH HHS/United States
- UL1 TR001872/TR/NCATS NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- UL1 TR002529/TR/NCATS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UL1 TR002494/TR/NCATS NIH HHS/United States
- UL1 TR002736/TR/NCATS NIH HHS/United States
- U54 GM115516/GM/NIGMS NIH HHS/United States
- UL1 TR002369/TR/NCATS NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- U54 GM115371/GM/NIGMS NIH HHS/United States
- UL1 TR002001/TR/NCATS NIH HHS/United States
- UL1 TR002538/TR/NCATS NIH HHS/United States
- U54 GM115458/GM/NIGMS NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- UL1 TR001866/TR/NCATS NIH HHS/United States
- UL1 TR003167/TR/NCATS NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- UL1 TR001453/TR/NCATS NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- UL1 TR003107/TR/NCATS NIH HHS/United States
- UL1 TR003015/TR/NCATS NIH HHS/United States
- UL1 TR002733/TR/NCATS NIH HHS/United States
- U24 TR002306/TR/NCATS NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
- UL1 TR001876/TR/NCATS NIH HHS/United States
- UL1 TR001436/TR/NCATS NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- UL1 TR002553/TR/NCATS NIH HHS/United States
- UL1 TR002389/TR/NCATS NIH HHS/United States
- UL1 TR001414/TR/NCATS NIH HHS/United States
- U54 GM104941/GM/NIGMS NIH HHS/United States
- UL1 TR002014/TR/NCATS NIH HHS/United States
- UL1 TR002550/TR/NCATS NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR001855/TR/NCATS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- UL1 TR002373/TR/NCATS NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- UL1 TR002556/TR/NCATS NIH HHS/United States
- UL1 TR003017/TR/NCATS NIH HHS/United States
- UL1 TR001998/TR/NCATS NIH HHS/United States
- UL1 TR001873/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR002645/TR/NCATS NIH HHS/United States
- UL1 TR001450/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- U54 GM115428/GM/NIGMS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- UL1 TR002377/TR/NCATS NIH HHS/United States
- U54 GM115677/GM/NIGMS NIH HHS/United States
- UL1 TR002544/TR/NCATS NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- UL1 TR001430/TR/NCATS NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
