

Inequities in surgical outcomes by race and sex in the United States: retrospective cohort study
- PMID: 36858422
- PMCID: PMC9975928
- DOI: 10.1136/bmj-2022-073290
Inequities in surgical outcomes by race and sex in the United States: retrospective cohort study
Abstract
Objective: To assess inequities in mortality by race and sex for eight common surgical procedures (elective and non-elective) across specialties in the United States.
Design: Retrospective cohort study.
Setting: US, 2016-18.
Participants: 1 868 036 Black and White Medicare beneficiaries aged 65-99 years undergoing one of eight common surgeries: repair of abdominal aortic aneurysm, appendectomy, cholecystectomy, colectomy, coronary artery bypass surgery, hip replacement, knee replacement, and lung resection.
Main outcome measure: The main outcome measure was 30 day mortality, defined as death during hospital admission or within 30 days of the surgical procedure.
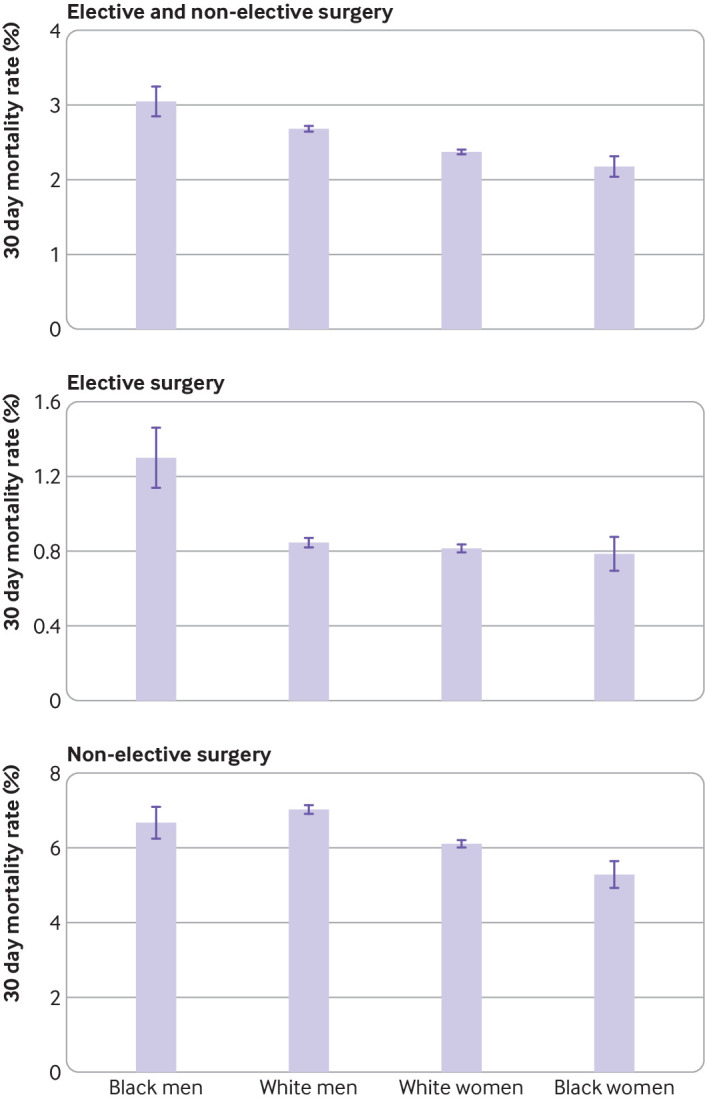
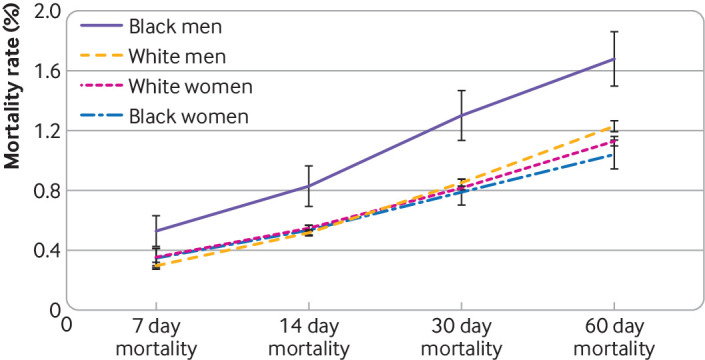
Results: Postoperative mortality overall was higher in Black men (1698 deaths, adjusted mortality rate 3.05%, 95% confidence interval 2.85% to 3.24%) compared with White men (21 833 deaths, 2.69%, 2.65% to 2.73%), White women (21 847 deaths, 2.38%, 2.35% to 2.41%), and Black women (1631 deaths, 2.18%, 2.04% to 2.31%), after adjusting for potential confounders. A similar pattern was found for elective surgeries, with Black men showing a higher adjusted mortality (393 deaths, 1.30%, 1.14% to 1.46%) compared with White men (5650 deaths, 0.85%, 0.83% to 0.88%), White women (4615 deaths, 0.82%, 0.80% to 0.84%), and Black women (359 deaths, 0.79%, 0.70% to 0.88%). This 0.45 percentage point difference implies that mortality after elective procedures was 50% higher in Black men compared with White men. For non-elective surgeries, however, mortality did not differ between Black men and White men (1305 deaths, 6.69%, 6.26% to 7.11%; and 16 183 deaths, 7.03%, 6.92% to 7.14%, respectively), although mortality was lower for White women and Black women (17 232 deaths, 6.12%, 6.02% to 6.21%; and 1272 deaths, 5.29%, 4.93% to 5.64%, respectively). These differences in mortality appeared within seven days after surgery and persisted for up to 60 days after surgery.
Conclusions: Postoperative mortality overall was higher among Black men compared with White men, White women, and Black women. These findings highlight the need to understand better the unique challenges Black men who require surgery face.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the National Institute on Minority Health and Health Disparities for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Racial disparities in abdominal aortic aneurysm repair among male Medicare beneficiaries.Arch Surg. 2008 May;143(5):506-10. doi: 10.1001/archsurg.143.5.506. Arch Surg. 2008. PMID: 18490563
-
Association of Medicare Mandatory Bundled Payment Program With the Receipt of Elective Hip and Knee Replacement in White, Black, and Hispanic Beneficiaries.JAMA Netw Open. 2021 Mar 1;4(3):e211772. doi: 10.1001/jamanetworkopen.2021.1772. JAMA Netw Open. 2021. PMID: 33749766 Free PMC article.
-
Association of Neighborhood Deprivation, Race, and Postoperative Outcomes: Improvement in Neighborhood Deprivation is Associated With Worsening Surgical Disparities.Ann Surg. 2023 Jun 1;277(6):958-963. doi: 10.1097/SLA.0000000000005475. Epub 2022 Jul 7. Ann Surg. 2023. PMID: 35797617
-
Fenestrated endovascular abdominal aortic aneurysm repair in octogenarians is associated with higher mortality and an increased incidence of nonhome discharge.J Vasc Surg. 2022 Jun;75(6):1846-1854.e7. doi: 10.1016/j.jvs.2022.01.076. Epub 2022 Jan 26. J Vasc Surg. 2022. PMID: 35090994 Review.
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
Cited by
-
Race based disparities in clinical and financial outcomes associated with major elective and emergent surgery.Surg Open Sci. 2025 Apr 29;26:39-46. doi: 10.1016/j.sopen.2025.04.010. eCollection 2025 Jun. Surg Open Sci. 2025. PMID: 40421313 Free PMC article.
-
Modifiable risk factors of inequalities in hypertension: analysis of 100 million health checkups recipients.Hypertens Res. 2024 Jun;47(6):1555-1566. doi: 10.1038/s41440-024-01615-9. Epub 2024 Mar 5. Hypertens Res. 2024. PMID: 38443615
-
Understanding the impact of racism on surgical outcomes in settler nation-states USA and Canada: a protocol for a systematic review and meta-analysis.BMJ Open. 2025 Jan 29;15(1):e086461. doi: 10.1136/bmjopen-2024-086461. BMJ Open. 2025. PMID: 39880426 Free PMC article.
-
No significant differences in 60-day postoperative complication rates between conventional and shortened stems.J Exp Orthop. 2023 Dec 28;10(1):149. doi: 10.1186/s40634-023-00696-8. J Exp Orthop. 2023. PMID: 38153605 Free PMC article.
-
Measuring hospital inpatient Procedure Access Inequality in the United States.Health Aff Sch. 2024 Nov 6;2(11):qxae142. doi: 10.1093/haschl/qxae142. eCollection 2024 Nov. Health Aff Sch. 2024. PMID: 39564567 Free PMC article.
References
-
- Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. 2003. https://www.ncbi.nlm.nih.gov/books/NBK220358/. - PubMed