Cerebrospinal Fluid Production and Absorption and Ventricular Enlargement Mechanisms in Hydrocephalus
- PMID: 36858632
- PMCID: PMC10166604
- DOI: 10.2176/jns-nmc.2022-0331
Cerebrospinal Fluid Production and Absorption and Ventricular Enlargement Mechanisms in Hydrocephalus
Abstract
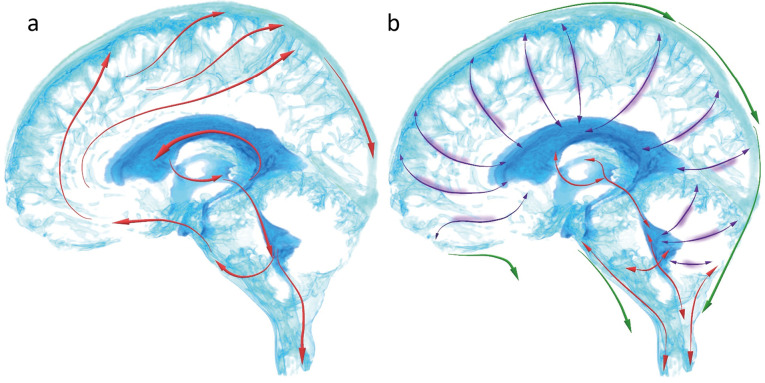
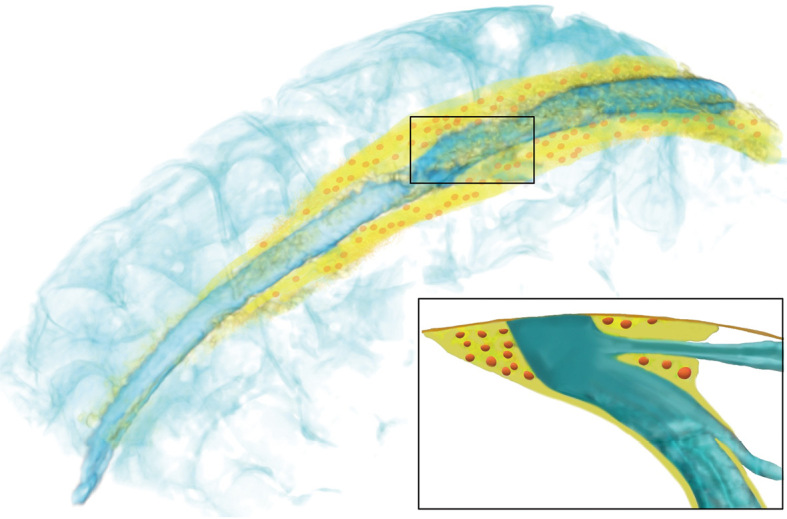
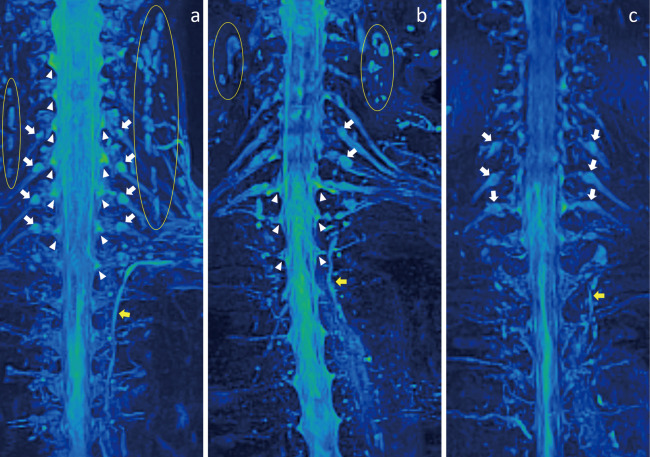
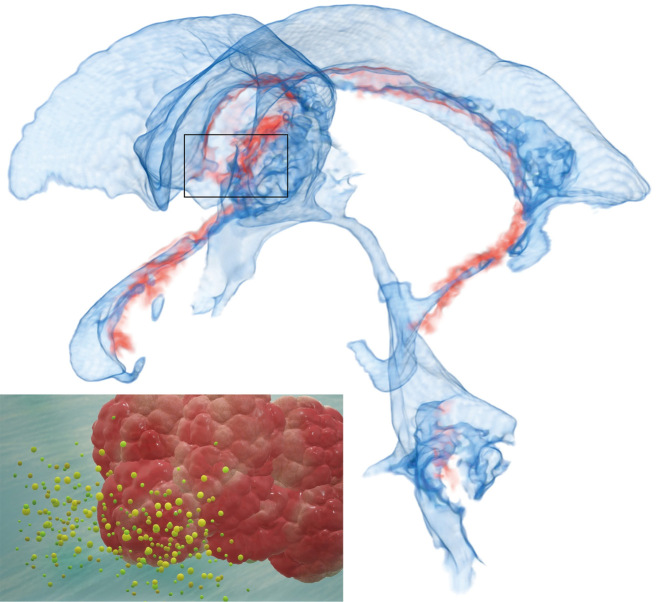
Cerebrospinal fluid (CSF) production and absorption concept significantly changed in the early 2010s from "third circulation theory" and "classical bulk flow theory" to a whole new one as follows: First, CSF is mainly produced from interstitial fluid excreted from the brain parenchyma, and CSF produced from the choroid plexus plays an important role in maintaining brain homeostasis. Second, CSF is not absorbed in the venous sinus via the arachnoid granules, but mainly in the dural lymphatic vessels. Finally, the ventricles and subarachnoid spaces have several compensatory direct CSF pathways at the borders attached to the choroid plexus, e.g., the inferior choroidal point of the choroidal fissure, other than the foramina of Luschka and Magendie. In idiopathic normal pressure hydrocephalus (iNPH), the lateral ventricles and basal cistern are enlarged simultaneously due to the compensatory direct CSF pathways. The average total intracranial CSF volume increased from about 150 mL at 20 years to about 350 mL at 70 years due to the decrease in brain volume with aging and further increased above 400 mL in patients with iNPH. CSF movements are composed of a steady microflow produced by the rhythmic wavy movement of motile cilia on the ventricular surface and dynamic pulsatile flow produced by the brain and cerebral artery pulsation, respiration, and head movement. Pulsatile CSF movements might totally decrease with aging, but it in the ventricles might increase at the foramina of Magendie and Luschka dilation. Aging CSF dynamics are strongly associated with ventricular dilatation in iNPH.
Keywords: cerebrospinal fluid dynamics; chronic hydrocephalus; ventricle dilatation.
Conflict of interest statement
All authors declare that they have no commercial or financial relationships of any kind that could be construed as potential conflicts of interest.
Figures