

The burden of illness in Lennox-Gastaut syndrome: a systematic literature review
- PMID: 36859290
- PMCID: PMC9979426
- DOI: 10.1186/s13023-023-02626-4
The burden of illness in Lennox-Gastaut syndrome: a systematic literature review
Abstract
Background: Lennox-Gastaut syndrome (LGS) is a severe developmental and epileptic encephalopathy characterized by drug-resistant epilepsy with multiple seizure types starting in childhood, a typical slow spike-wave pattern on electroencephalogram, and cognitive dysfunction.
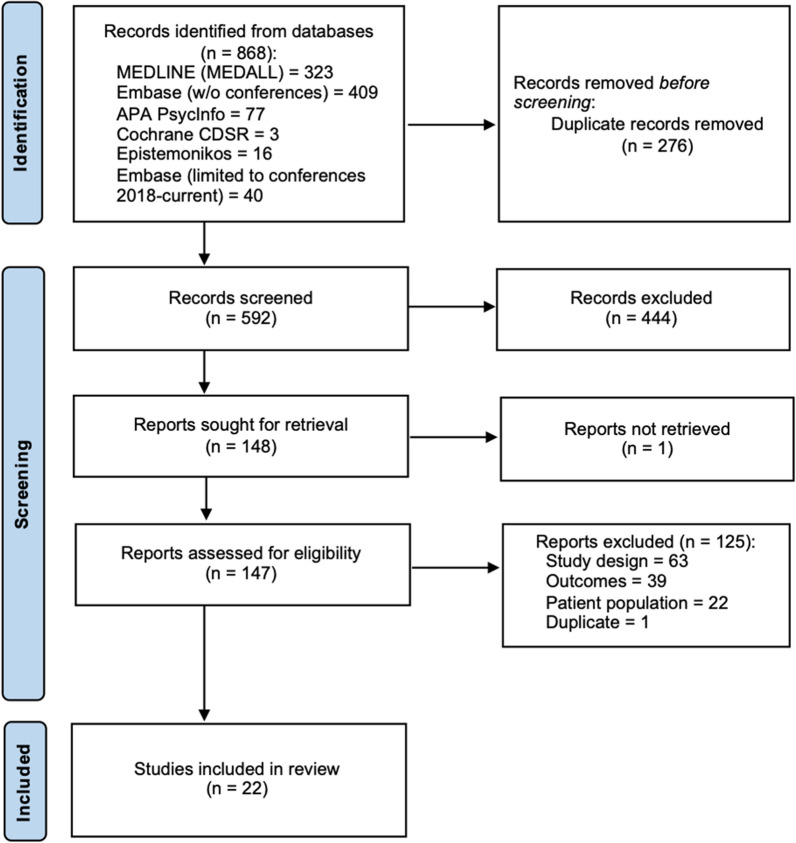
Methods: We performed a systematic literature review according to the PRISMA guidelines to identify, synthesize and appraise the burden of illness in LGS (including "probable" LGS). Studies were identified by searching MEDLINE, Embase and APA PsychInfo, Cochrane's database of systematic reviews, and Epistemonikos. The outcomes were epidemiology (incidence, prevalence or mortality), direct and indirect costs, healthcare resource utilization, and patient and caregiver health-related quality of life (HRQoL).
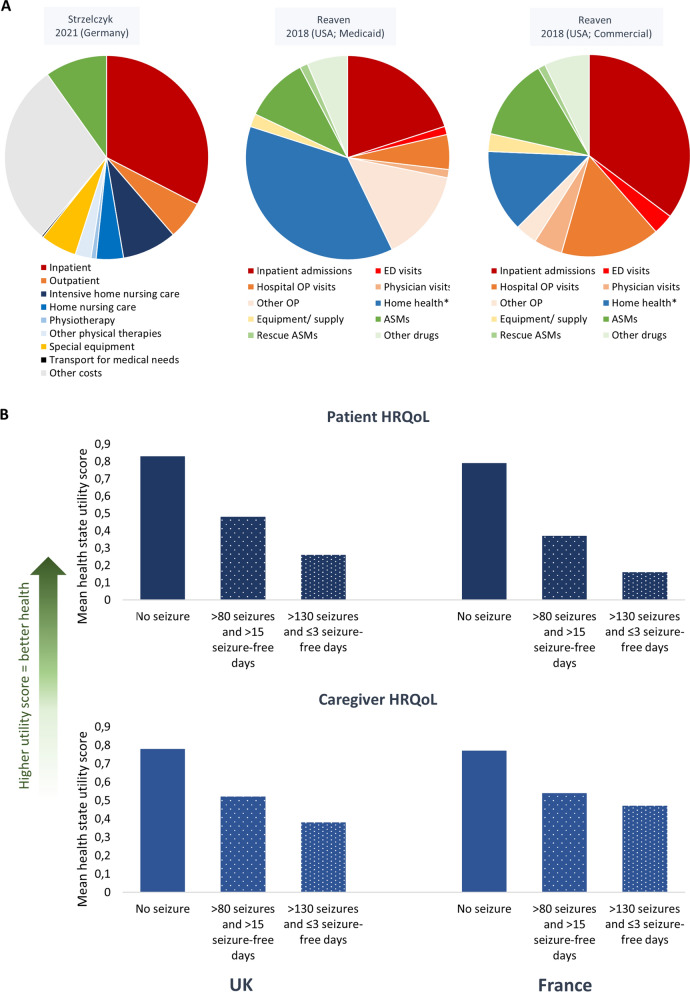
Results: The search identified 22 publications evaluating the epidemiology (n = 10), direct costs and resource (n = 10) and/or HRQoL (n = 5). No studies reporting on indirect costs were identified. With no specific ICD code for LGS in many regions, several studies had to rely upon indirect methods to identify their patient populations (e.g., algorithms to search insurance claims databases to identify "probable" LGS). There was heterogeneity between studies in how LGS was defined, the size of the populations, ages of the patients and length of the follow-up period. The prevalence varied from 4.2 to 60.8 per 100,000 people across studies for probable LGS and 2.9-28 per 100,000 for a confirmed/narrow definition of LGS. LGS was associated with high mortality rates compared to the general population and epilepsy population. Healthcare resource utilization and direct costs were substantial across all studies. Mean annual direct costs per person varied from $24,048 to $80,545 across studies, and home-based care and inpatient care were significant cost drivers. Studies showed that the HRQoL of patients and caregivers was adversely affected, although only a few studies were identified. In addition, studies suggested that seizure events were associated with higher costs and worse HRQoL. The risk of bias was low or moderate in most studies.
Conclusions: LGS is associated with a significant burden of illness featuring resistant seizures associated with higher costs and worse HRQoL. More research is needed, especially in evaluating indirect costs and caregiver burden, where there is a notable lack of studies.
Keywords: Burden of illness; Caregiver burden; Developmental and epileptic encephalopathy; Direct costs; Epilepsy; Health-related quality of life; Indirect costs; Lennox–Gastaut syndrome; Seizures.
© 2023. The Author(s).
Conflict of interest statement
AS reports personal fees and grants from Angelini Pharma, Desitin Arzneimittel, Eisai, Jazz/GW Pharmaceuticals companies, Marinus Pharma, Precisis, Takeda, UCB, UNEEG medical, and Zogenix. SZ reports research support from Epilepsy Research UK, Scottish Government Digital Health & Care, UCB Pharma, Dravet Syndrome UK, Dravet Syndrome Foundation, Tenovus Foundation and Glasgow Children’s Hospital Charity. He or his institution have received honoraria for consultancy work, educational symposia and advisory boards from GW Pharma, Zogenix, UCB, Encoded Therapeutics, Takeda and Eisai. PS reports personal fees and grants from Angelini Pharma, Eisai, Jazz Pharmaceuticals Biomarin, UCB, Proveca, and Zogenix. FR reports personal fees from Angelini Pharma, Arvelle Therapeutics, Eisai GmbH, GW Pharmaceuticals companies, and UCB and grants from the Detlev-Wrobel-Fonds for Epilepsy Research, the Deutsche Forschungsgemeinschaft, the LOEWE Programme of the State of Hesse, and the European Union. SSB reports personal fees from Eisai, Desitin Pharma, GW Pharmaceuticals companies, Ethypharm, UCB, and Zogenix.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
