

A suture anchor-based repair technique for type IV jersey finger injuries: a biomechanical investigation
- PMID: 36859502
- PMCID: PMC9978029
- DOI: 10.1038/s41598-023-30373-w
A suture anchor-based repair technique for type IV jersey finger injuries: a biomechanical investigation
Abstract
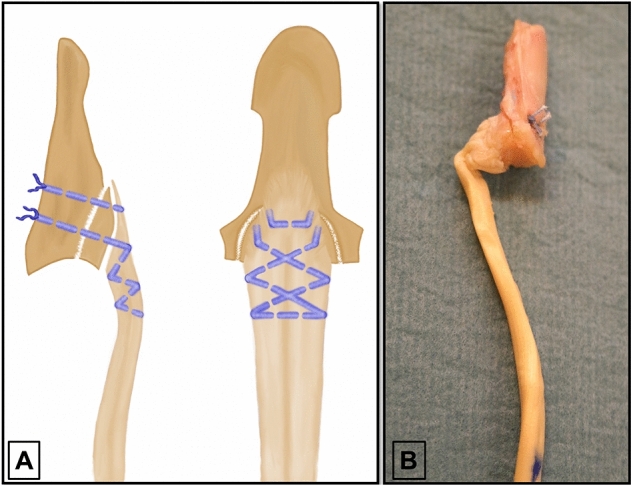
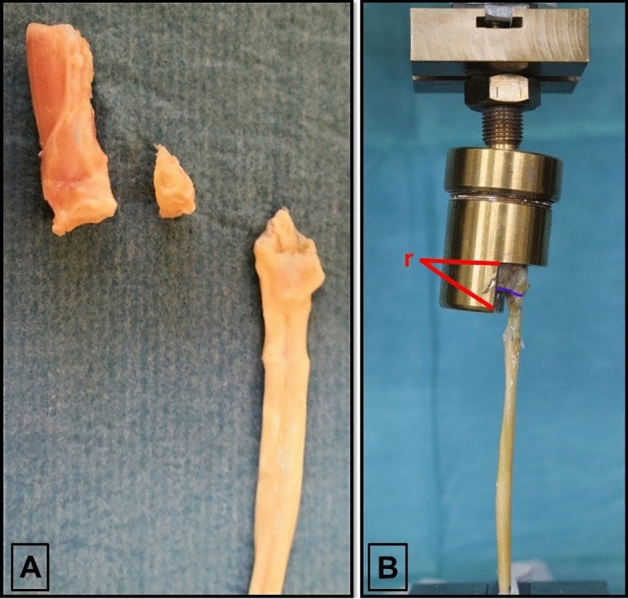
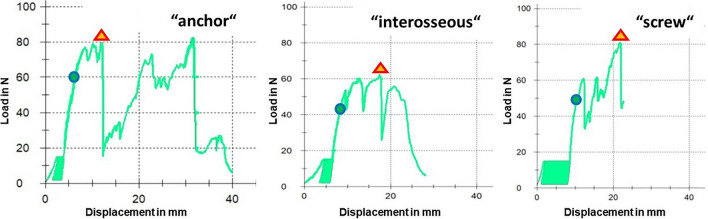
The aim of this biomechanical investigation was to evaluate a repair technique for type IV FDP tendon avulsions using a suture anchor, addressing the bony and the tendinous aspect of this injury simultaneously. In 45 distal phalanges from human anatomical specimens the injury was simulated and repairs were performed with a suture anchor using an innovative technique, interosseous sutures and a combination of screws and an interosseous suture. Repetitive loading for 500 cycles simulated postoperative mobilization. Repairs were loaded to failure thereafter. Elongation of the tendon-suture complex, gap formation at the bone-bone contact line and at the bone-tendon insertion line, load at first noteworthy displacement (2 mm), load at failure and the mechanism of failure were assessed. The suture anchor technique was superior biomechanically considering load at failure (mean: 72.8 N), bony gap formation (mean: 0.1 mm) as well as tendinous gap formation (mean: 0.7 mm), implying a preferable stability of the repair. Overall, this study demonstrates good ex vivo mechanical stability for a proposed suture anchor repair technique for type IV FDP tendon avulsion injuries, which might enable early postoperative mobilization in patients. The technique's subcutaneous implant placement and low implant load are expected to reduce potential complications observed in other commonly used repair techniques. This approach warrants further evaluation in vivo.
© 2023. The Author(s).
Conflict of interest statement
The implants used in all study groups in this manuscript were provided by Arthex GmbH, Munich, Germany, following an Investigator - Initiated Research Agreement. As all used implants were provided by the same company, we believe that objectivity, integrity and the value of the results were preserved. No financial support, nor any other non - financial benefits were, or will be recieved. The authors declare no competing interest.
Figures


References
-
- Robins, P. R. Avulsion of the insertion of the flexor digitorum profundus tendon associated with fracture of the distal phalanx. In A. A. O. S. Symposium on Tendon Surgery in the Hand 151–156 (1975).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
