

[18F]FDG PET/CT versus [18F]FDG PET/MRI for the diagnosis of colorectal liver metastasis: A systematic review and meta-analysis
- PMID: 36860315
- PMCID: PMC9969139
- DOI: 10.3389/fonc.2023.1114059
[18F]FDG PET/CT versus [18F]FDG PET/MRI for the diagnosis of colorectal liver metastasis: A systematic review and meta-analysis
Abstract
Purpose: The purpose of our meta-analysis and systematic review was to compare the diagnostic performance of [18F]FDG PET/CT and [18F]FDG PET/MRI in colorectal liver metastasis.
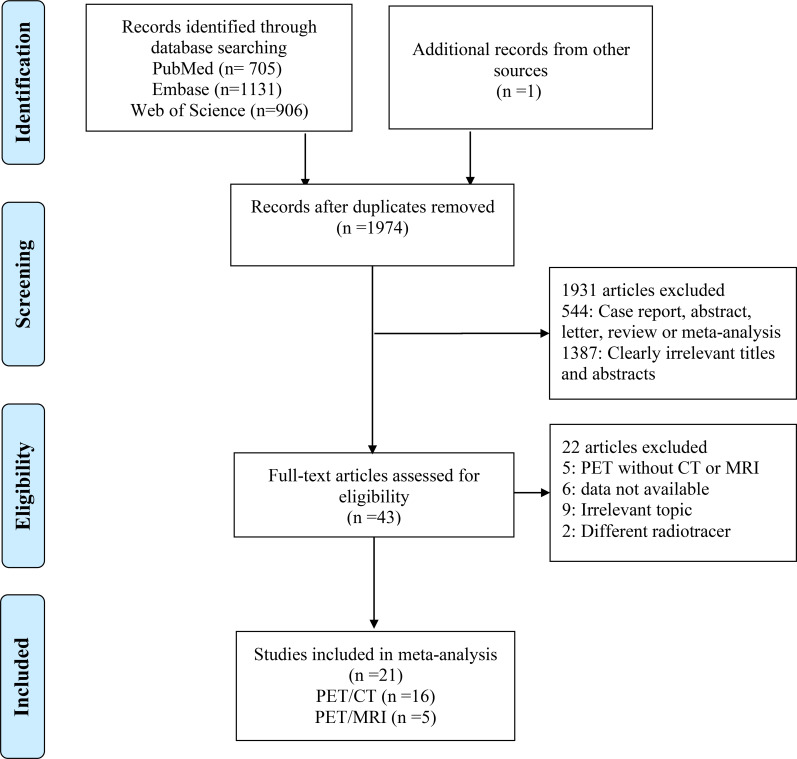
Methods: We searched PubMed, Embase, and Web of Science for eligible articles until November 2022. Studies focusing on the diagnostic value of [18F]FDG PET/CT or PET/MRI for colorectal liver metastasis were included. Using a bivariate random-effect model, the pooled sensitivity and specificity for [18F]FDG PET/CT and [18F]FDG PET/MRI were reported as estimates with 95% confidence intervals (CIs). Heterogeneity among pooled studies was assessed using the I2 statistic. The Quality Assessment of Diagnostic Performance Studies (QUADAS-2) method was used to evaluate the quality of the studies that were included.
Results: There were a total of 2743 publications identified in the initial search, finally, a total of 21 studies comprising 1036 patients were included. The pooled sensitivity, specificity, and AUC of [18F]FDG PET/CT in were 0.86 (95% CI: 0.76-0.92), 0.89 (95% CI: 0.83-0.94), and 0.92(95% CI: 0.90-0.94). [18F]FDG PET/MRI were 0.84 (95% CI: 0.77-0.89), 1.00 (95% CI: 0.32-1.00), and 0.89(95% CI: 0.86-0.92), respectively.
Conclusion: [18F]FDG PET/CT shows similar performance compared to [18F]FDG PET/MRI in detecting colorectal liver metastasis. However, pathological results were not obtained for all patients in the included studies and PET/MRI results were derived from studies with small sample sizes. There is a need for additional, larger prospective studies on this issue.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier (CRD42023390949).
Keywords: PET/CT; PET/MRI; colorectal neoplasms; liver metastasis; meta-analysis.
Copyright © 2023 Miao, Zhao and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







Similar articles
-
[18F]FDG PET/CT versus [18F]FDG PET/MRI in staging of non-small cell lung cancer: a head-to-head comparative meta-analysis.Front Med (Lausanne). 2025 Jan 13;11:1517805. doi: 10.3389/fmed.2024.1517805. eCollection 2024. Front Med (Lausanne). 2025. PMID: 39871837 Free PMC article.
-
[18F]FDG PET/CT versus [18F]FDG PET/MRI in the diagnosis of lymph node metastasis in nasopharyngeal carcinoma: a systematic review and meta-analysis.Front Med (Lausanne). 2024 Oct 16;11:1450526. doi: 10.3389/fmed.2024.1450526. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39478819 Free PMC article.
-
18F-FDG PET/CT and whole-body MRI diagnostic performance in M staging for non-small cell lung cancer: a systematic review and meta-analysis.Eur Radiol. 2020 Jul;30(7):3641-3649. doi: 10.1007/s00330-020-06703-1. Epub 2020 Mar 3. Eur Radiol. 2020. PMID: 32125513
-
Head-to-head comparison of 68Ga-FAPI-04 PET/CT and 18F-FDG PET/CT in the evaluation of primary digestive system cancer: a systematic review and meta-analysis.Front Oncol. 2023 Jun 26;13:1202505. doi: 10.3389/fonc.2023.1202505. eCollection 2023. Front Oncol. 2023. PMID: 37434980 Free PMC article.
-
Comparison of whole-body 18F-FDG PET/CT and PET/MRI for distant metastases in patients with malignant tumors: a meta-analysis.BMC Cancer. 2023 Jan 10;23(1):37. doi: 10.1186/s12885-022-10493-8. BMC Cancer. 2023. PMID: 36624425 Free PMC article.
Cited by
-
Colorectal cancer liver metastases: A radiologic point of view.World J Gastrointest Oncol. 2025 Aug 15;17(8):103473. doi: 10.4251/wjgo.v17.i8.103473. World J Gastrointest Oncol. 2025. PMID: 40837779 Free PMC article.
References
-
- Artigas Martín JM, Alonso Orduña V, Serrablo Requejo A, Larrosa López R, Martín Cuartero J. Epidemiology and diagnosis of liver metastases. Revisiones en Cancer (2008) 22(1):1–13.
-
- Manfredi S, Lepage C, Hatem C, Coatmeur O, Faivre J, Bouvier AM. Epidemiology and management of liver metastases from colorectal cancer. Ann Surg (2006) 244(2):254–9. doi: 10.1097/01.sla.0000217629.94941.cf - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources