

Morphea: The 2023 update
- PMID: 36860340
- PMCID: PMC9969991
- DOI: 10.3389/fmed.2023.1108623
Morphea: The 2023 update
Abstract
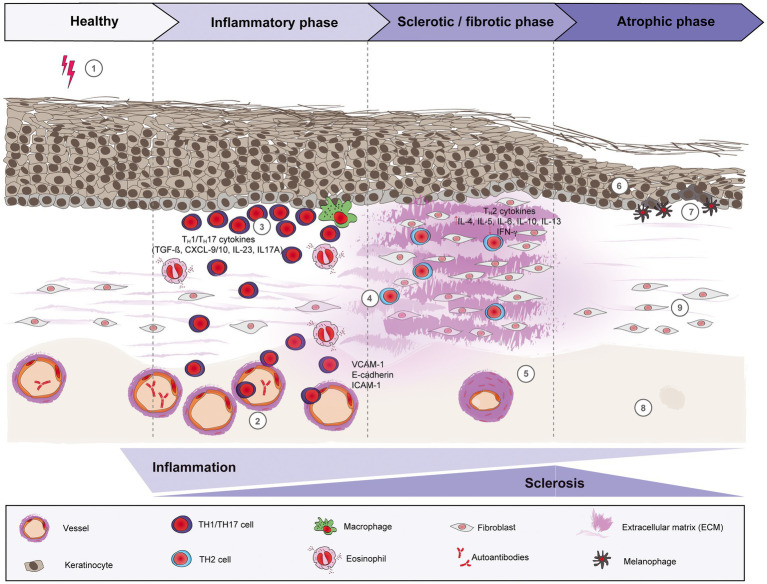
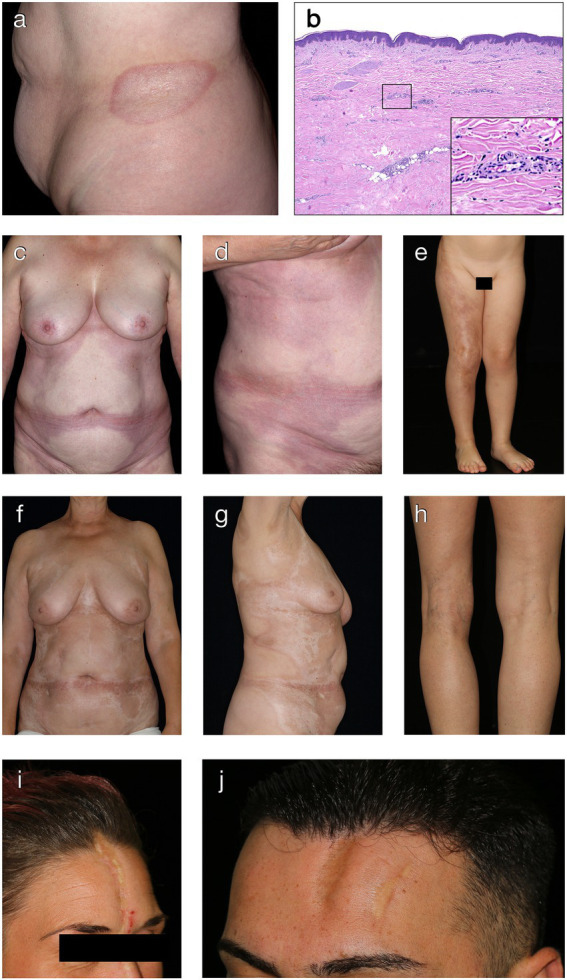
Morphea, also known as localized scleroderma, is a chronic inflammatory connective tissue disorder with variable clinical presentations, that affects both adults and children. It is characterized by inflammation and fibrosis of the skin and underlying soft tissue, in certain cases even of the surrounding structures such as fascia, muscle, bone and central nervous system. While the etiology is still unknown, many factors may contribute to disease development, including genetic predisposition, vascular dysregulation, TH1/TH2 imbalance with chemokines and cytokines associated with interferon-γ and profibrotic pathways as well as certain environmental factors. Since the disease may progress to permanent cosmetic and functional sequelae, it is crucial to properly assess the disease activity and to initiate promptly the adequate treatment, thus preventing subsequent damage. The mainstay of treatment is based on corticosteroids and methotrexate. These, however, are limited by their toxicity, especially if applied long-term. Furthermore, corticosteroids and methotrexate often do not sufficiently control the disease and/or the frequent relapses of morphea. This review presents the current understanding of morphea by discussing its epidemiology, diagnosis, management and prognosis. In addition, it will describe recent pathogenetic findings, thus proposing potential novel targets for therapeutic development in morphea.
Keywords: diagnosis; localized scleroderma; morphea; pathogenesis; treatment.
Copyright © 2023 Papara, De Luca, Bieber, Vorobyev and Ludwig.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources