

Right ventricular outflow tract stenting promotes pulmonary artery development in tetralogy of fallot
- PMID: 36860944
- PMCID: PMC9968738
- DOI: 10.3389/fsurg.2023.1056772
Right ventricular outflow tract stenting promotes pulmonary artery development in tetralogy of fallot
Abstract
Background: Right ventricular outflow tract (RVOT) stenting seems to be suggested as a promising treatment option and an alternative to modified Blalock-Taussig shunt (mBTS) in the initial palliation of patients with Fallot-type lesions in recent years. This study sought to assess the effect of RVOT stenting on the growth of the pulmonary artery (PA) in patients with Tetralogy of Fallot (TOF).
Methods: Retrospective review analyzing 5 patients with Fallot-type congenital heart disease with small pulmonary arteries who underwent palliative with RVOT stenting and 9 patients underwent modified Blalock-Taussig shunt within 9 years period. Differential left PA (LPA) and right PA (RPA) growth was measured by Cardiovascular Computed Tomography Angiography (CTA).
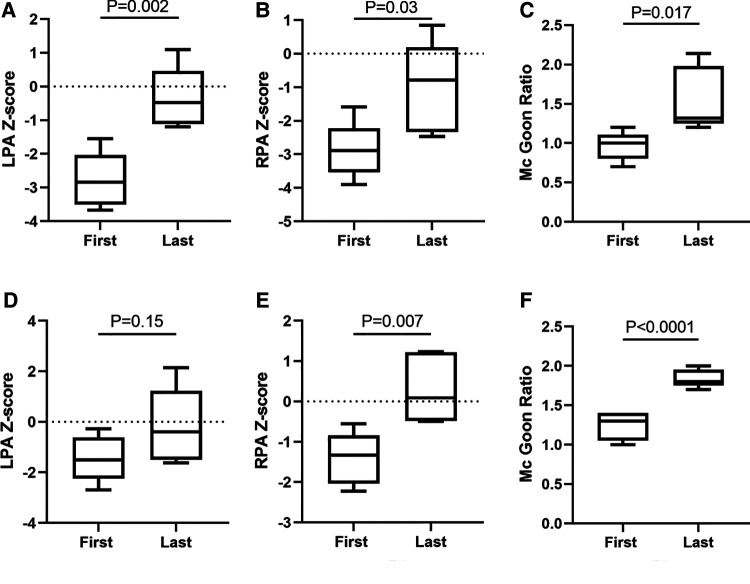
Results: RVOT stenting improved arterial oxygen saturation from median of 60% (interquartile range [IQR]: 37% to 79%) to 95% (87.5% to 97.5%) (p = 0.028). The LPA diameter Z-score improved from -2.843 (-3.51-2.037) to -0.78 (-2.3305-0.19) (p = 0.03), the RPA diameter Z-score improved from median -2.843 (-3.51-2.037) to -0.477 (-1.1145-0.459) (p = 0.002), the Mc Goon ratio increased from median 1 (0.8-1.105) to 1.32 (1.25-1.98) (p = 0.017). There were no procedural complications and all 5 patients have undergone final repair in the RVOT stent group. In the mBTS group, the LPA diameter Z-score improved from -1.494 (-2.242-0.6135) to -0.396 (-1.488-1.228) (p = 0.15), the RPA diameter Z-score improved from median -1.328 (-2.036-0.838) to 0.088 (-0.486-1.223) (p = 0.007), and there were 5 patients occur different complications and 4 patients was not attained the standards of final surgical repair.
Conclusion: RVOT stenting, compared with mBTS, seems to better promote pulmonary artery growth, improve arterial oxygen saturations, and have less procedure complications in patients with TOF who being absolute contraindicated for primary repair due to high risks.
Keywords: oxygen saturation; primary palliation; pulmonary artery; right ventricular outflow tract stent; tetralogy of fallot.
© 2023 Guo, Wu, Zhao, Jinfu, Hu, Huang, Yang and Xie.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Stenting of the Right Ventricular Outflow Tract Promotes Better Pulmonary Arterial Growth Compared With Modified Blalock-Taussig Shunt Palliation in Tetralogy of Fallot-Type Lesions.JACC Cardiovasc Interv. 2017 Sep 11;10(17):1774-1784. doi: 10.1016/j.jcin.2017.06.023. JACC Cardiovasc Interv. 2017. PMID: 28882285
-
Surgical repair of Tetralogy of Fallot following primary palliation: Right ventricular outflow track stenting versus modified Blalock-Taussig shunt.Indian Heart J. 2018 Dec;70 Suppl 3(Suppl 3):S394-S398. doi: 10.1016/j.ihj.2018.06.020. Epub 2018 Jun 24. Indian Heart J. 2018. PMID: 30595296 Free PMC article.
-
Comparison between the modified Blalock-Taussig shunt and right ventricular outflow tract stent in the palliative treatment for tetralogy of Fallot.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 Sept 28;48(9):1325-1332. doi: 10.11817/j.issn.1672-7347.2023.230105. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 38044643 Free PMC article. Chinese, English.
-
Clinical Outcome of Right Ventricular Outflow Tract Stenting Versus Blalock-Taussig Shunt in Tetralogy of Fallot: A systematic Review and Meta-Analysis.Curr Probl Cardiol. 2021 Mar;46(3):100643. doi: 10.1016/j.cpcardiol.2020.100643. Epub 2020 Jun 4. Curr Probl Cardiol. 2021. PMID: 32773127
-
Right Ventricular Outflow Tract Stenting is a Safe and Effective Bridge to Definitive Repair in Symptomatic Infants With Tetralogy of Fallot1.Heart Lung Circ. 2023 May;32(5):638-644. doi: 10.1016/j.hlc.2023.02.010. Epub 2023 Mar 22. Heart Lung Circ. 2023. PMID: 36964005 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous