

Reversal of Lactate and PD-1-mediated Macrophage Immunosuppression Controls Growth of PTEN/p53-deficient Prostate Cancer
- PMID: 36862086
- PMCID: PMC10192075
- DOI: 10.1158/1078-0432.CCR-22-3350
Reversal of Lactate and PD-1-mediated Macrophage Immunosuppression Controls Growth of PTEN/p53-deficient Prostate Cancer
Abstract
Purpose: Phosphatase and tensin homolog (PTEN) loss of function occurs in approximately 50% of patients with metastatic castrate-resistant prostate cancer (mCRPC), and is associated with poor prognosis and responsiveness to standard-of-care therapies and immune checkpoint inhibitors. While PTEN loss of function hyperactivates PI3K signaling, combinatorial PI3K/AKT pathway and androgen deprivation therapy (ADT) has demonstrated limited anticancer efficacy in clinical trials. Here, we aimed to elucidate mechanism(s) of resistance to ADT/PI3K-AKT axis blockade, and to develop rational combinatorial strategies to effectively treat this molecular subset of mCRPC.
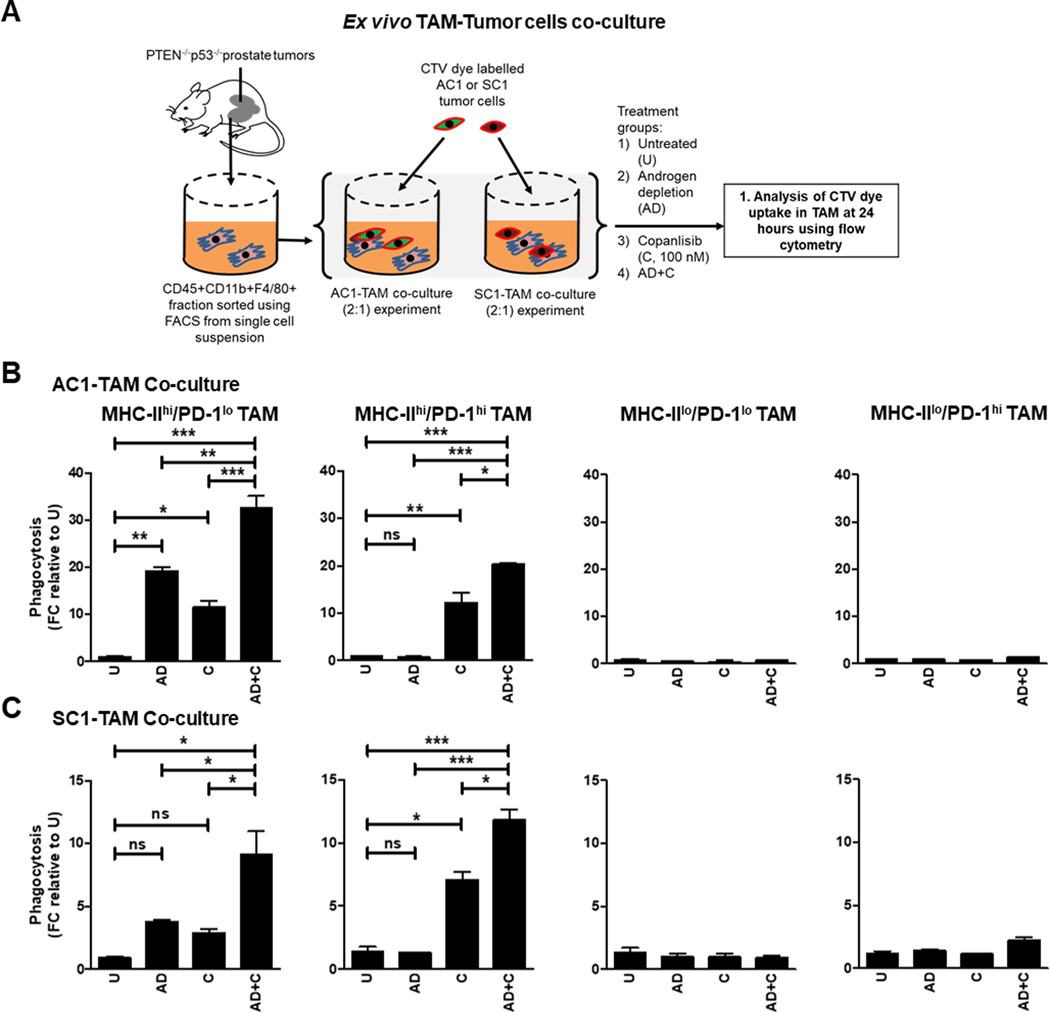
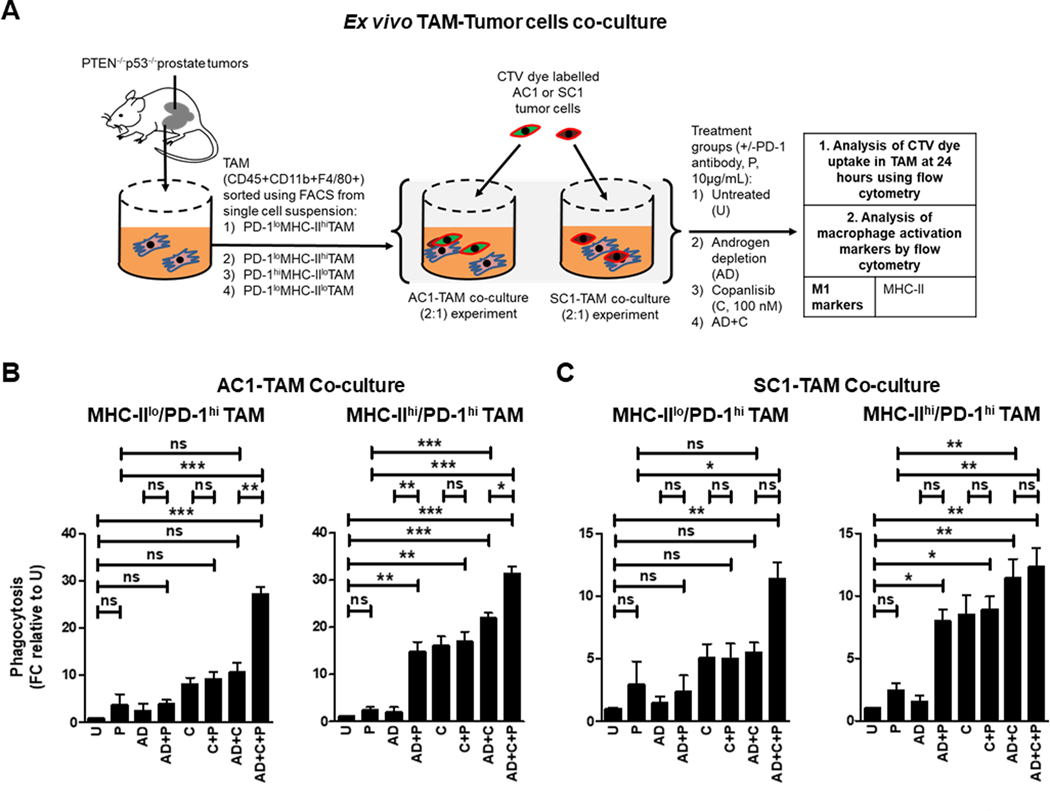
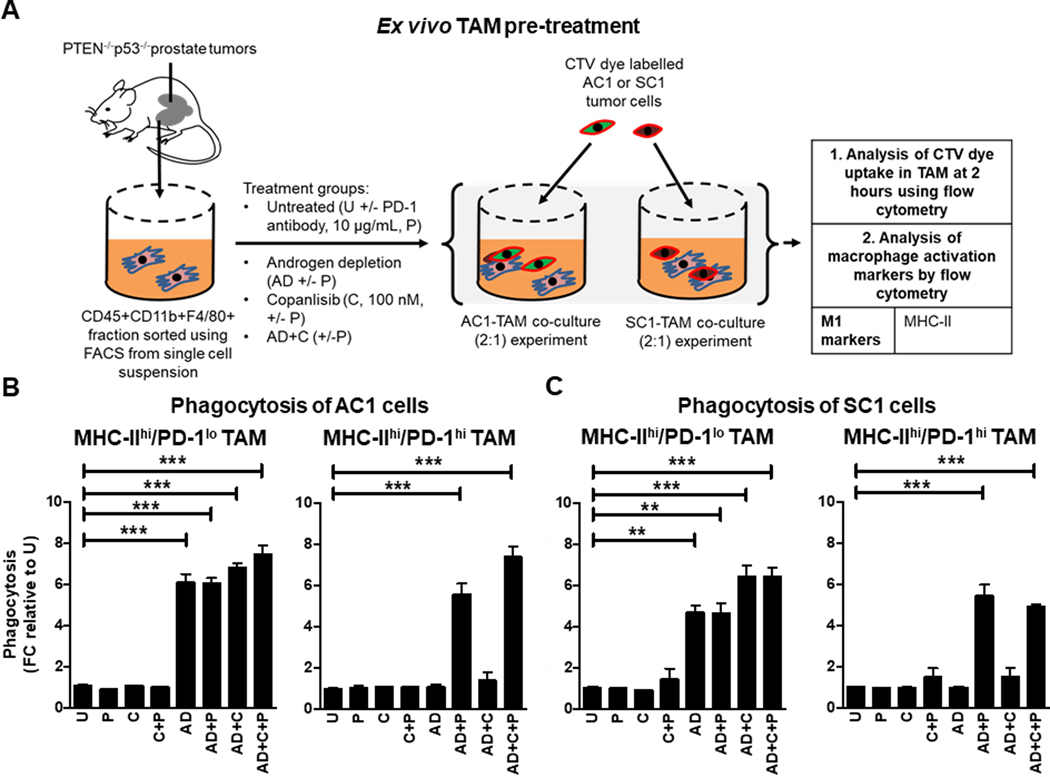
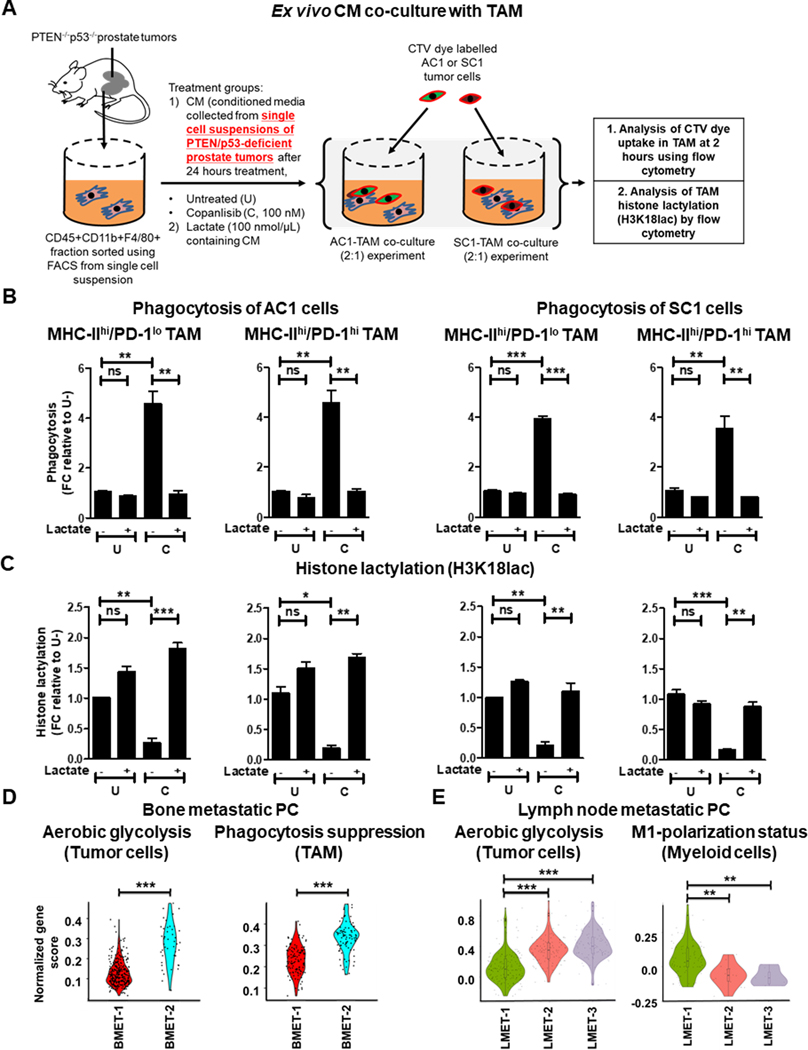
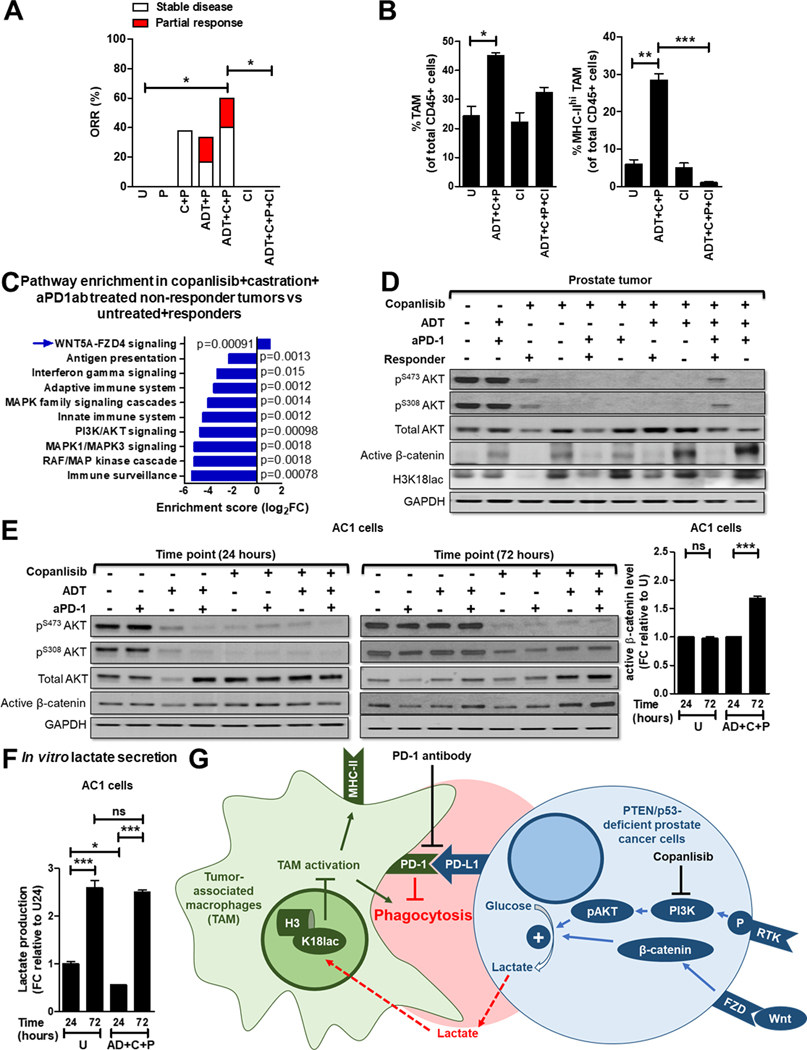
Experimental design: Prostate-specific PTEN/p53-deficient genetically engineered mice (GEM) with established 150-200 mm3 tumors, as assessed by ultrasound, were treated with either ADT (degarelix), PI3K inhibitor (copanlisib), or anti-PD-1 antibody (aPD-1), as single agents or their combinations, and tumors were monitored by MRI and harvested for immune, transcriptomic, and proteomic profiling, or ex vivo co-culture studies. Single-cell RNA sequencing on human mCRPC samples was performed using 10X Genomics platform.
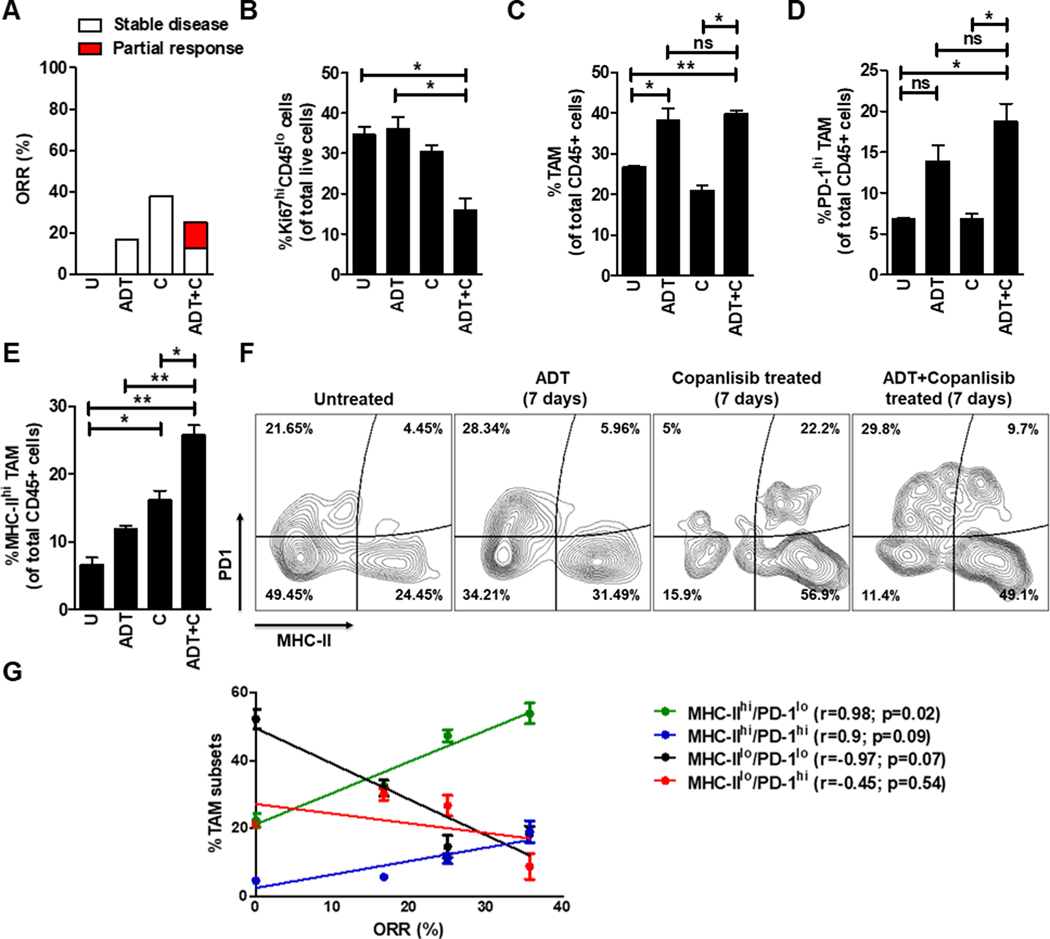
Results: Coclinical trials in PTEN/p53-deficient GEM revealed that recruitment of PD-1-expressing tumor-associated macrophages (TAM) thwarts ADT/PI3Ki combination-induced tumor control. The addition of aPD-1 to ADT/PI3Ki combination led to TAM-dependent approximately 3-fold increase in anticancer responses. Mechanistically, decreased lactate production from PI3Ki-treated tumor cells suppressed histone lactylation within TAM, resulting in their anticancer phagocytic activation, which was augmented by ADT/aPD-1 treatment and abrogated by feedback activation of Wnt/β-catenin pathway. Single-cell RNA-sequencing analysis in mCRPC patient biopsy samples revealed a direct correlation between high glycolytic activity and TAM phagocytosis suppression.
Conclusions: Immunometabolic strategies that reverse lactate and PD-1-mediated TAM immunosuppression, in combination with ADT, warrant further investigation in patients with PTEN-deficient mCRPC.
©2023 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Sydes MR, Spears MR, Mason MD, Clarke NW, Dearnaley DP, de Bono JS, et al. Adding abiraterone or docetaxel to long-term hormone therapy for prostate cancer: directly randomised data from the STAMPEDE multi-arm, multi-stage platform protocol. Ann Oncol 2018;29(5):1235–48 doi 10.1093/annonc/mdy072. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
