

First-line Systemic Treatment Options for Metastatic Castration-Sensitive Prostate Cancer: A Living Systematic Review and Network Meta-analysis
- PMID: 36862387
- PMCID: PMC9982744
- DOI: 10.1001/jamaoncol.2022.7762
First-line Systemic Treatment Options for Metastatic Castration-Sensitive Prostate Cancer: A Living Systematic Review and Network Meta-analysis
Abstract
Importance: The effectiveness of triplet therapy compared with androgen pathway inhibitor (API) doublets in a heterogeneous patient population with metastatic castration-sensitive prostate cancer (mCSPC) is unknown.
Objective: To assess the comparative effectiveness of contemporary systemic treatment options for patients with mCSPC across clinically relevant subgroups.
Data sources: For this systematic review and meta-analysis, Ovid MEDLINE and Embase were searched from each database's inception (MEDLINE, 1946; Embase, 1974) through June 16, 2021. Subsequently, a "living" auto search was created with weekly updates to identify new evidence as it became available.
Study selection: Phase 3 randomized clinical trials (RCTs) assessing first-line treatment options for mCSPC.
Data extraction and synthesis: Two independent reviewers extracted data from eligible RCTs. The comparative effectiveness of different treatment options was assessed with a fixed-effect network meta-analysis. Data were analyzed on July 10, 2022.
Main outcomes and measures: Outcomes of interest included overall survival (OS), progression-free survival (PFS), grade 3 or higher adverse events, and health-related quality of life.
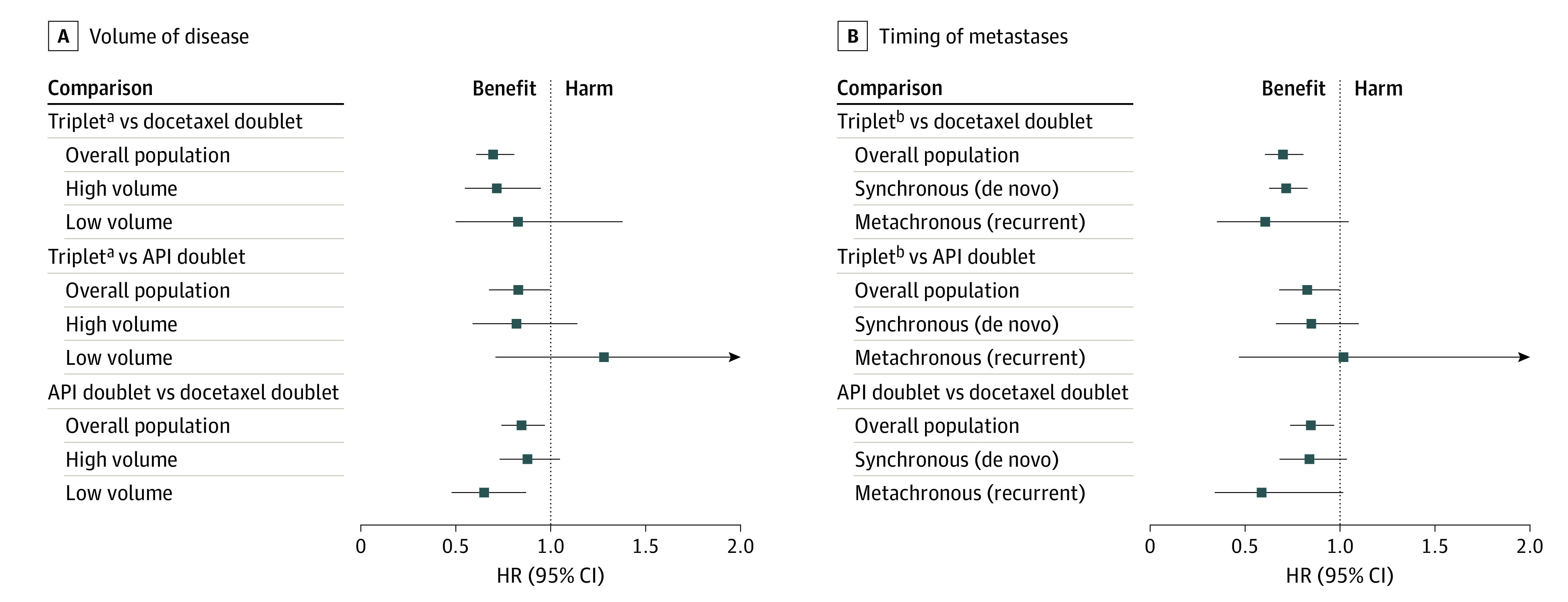
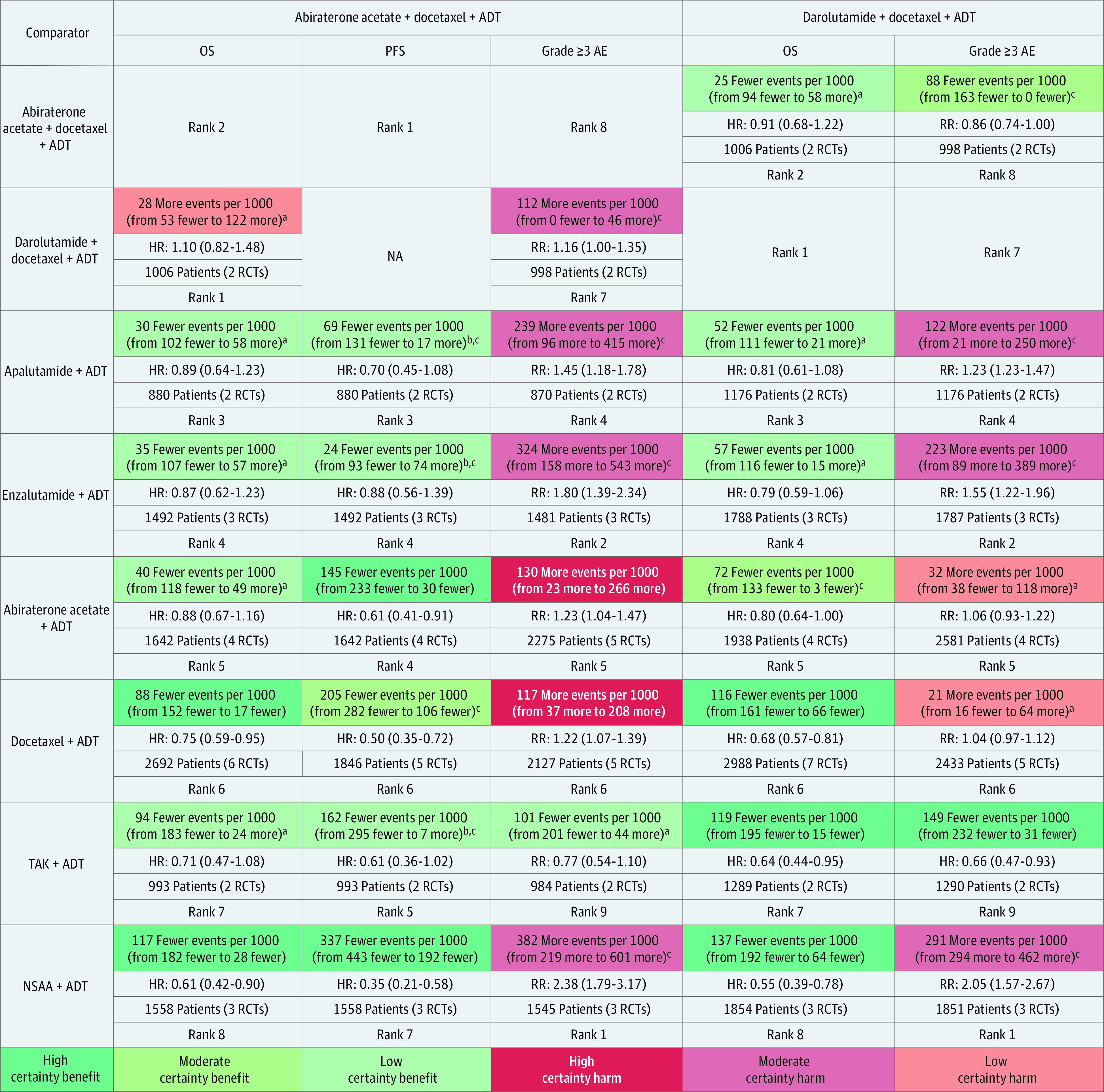
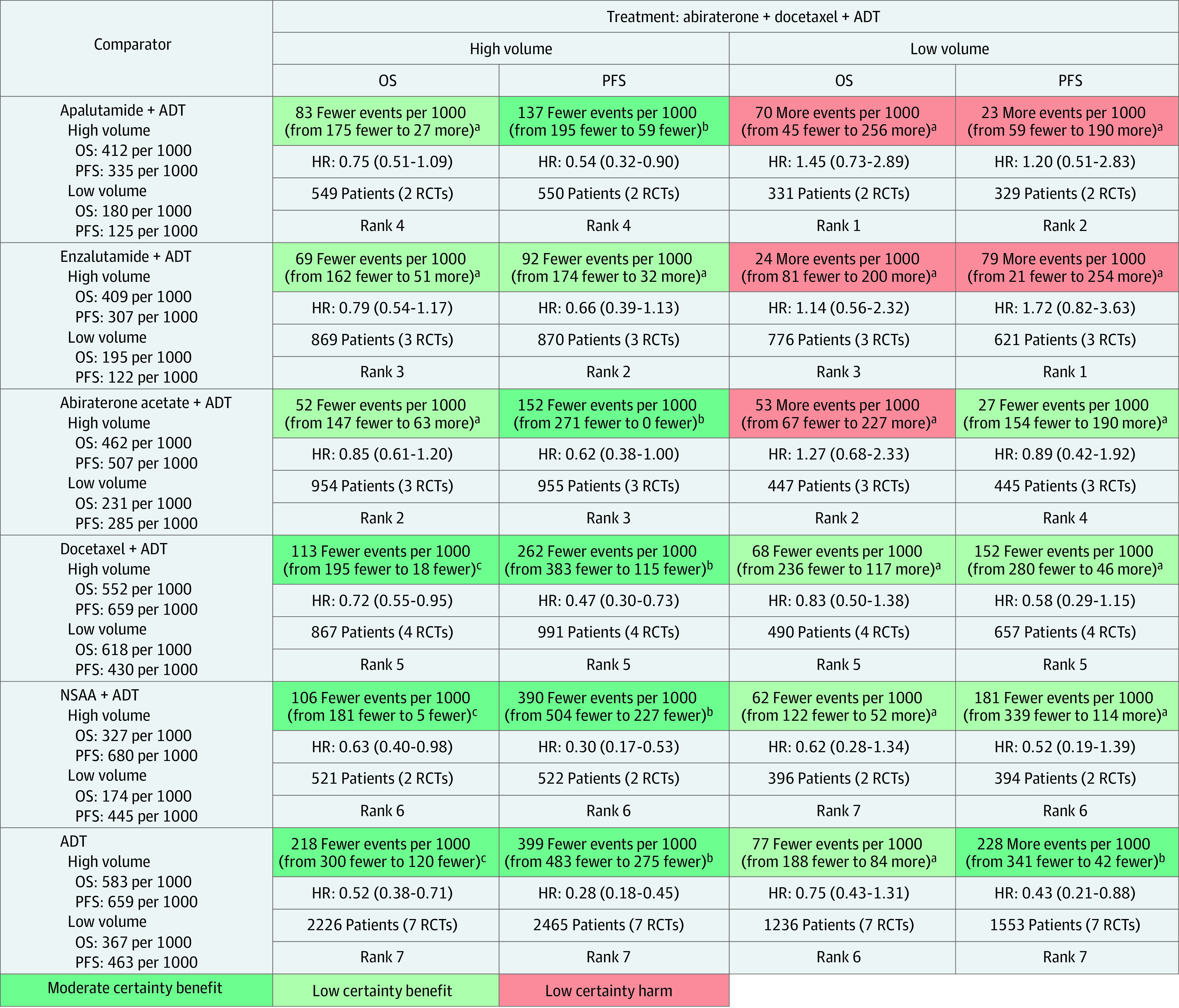
Results: This report included 10 RCTs with 11 043 patients and 9 unique treatment groups. Median ages of the included population ranged from 63 to 70 years. Current evidence for the overall population suggests that the darolutamide (DARO) triplet (DARO + docetaxel [D] + androgen deprivation therapy [ADT]; hazard ratio [HR], 0.68; 95% CI, 0.57-0.81), as well as the abiraterone (AAP) triplet (AAP + D + ADT; HR, 0.75; 95% CI, 0.59-0.95), are associated with improved OS compared with D doublet (D + ADT) but not compared with API doublets. Among patients with high-volume disease, AAP + D + ADT may improve OS compared with D + ADT (HR, 0.72; 95% CI, 0.55-0.95) but not compared with AAP + ADT, enzalutamide (E) + ADT, and apalutamide (APA) + ADT. For patients with low-volume disease, AAP + D + ADT may not improve OS compared with APA + ADT, AAP + ADT, E + ADT, and D + ADT.
Conclusions and relevance: The potential benefit observed with triplet therapy must be interpreted with careful accounting for the volume of disease and the choice of doublet comparisons used in the clinical trials. These findings suggest an equipoise to how triplet regimens compare with API doublet combinations and provide direction for future clinical trials.
Conflict of interest statement
Figures
Comment in
-
Triplet Therapy in Metastatic Hormone-Sensitive Prostate Cancer-Calling Out the "Double Standard".JAMA Oncol. 2023 May 1;9(5):617-619. doi: 10.1001/jamaoncol.2023.0324. JAMA Oncol. 2023. PMID: 36862389 No abstract available.
References
-
- Davis ID, Martin AJ, Stockler MR, et al. ; ENZAMET Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group . Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121-131. doi:10.1056/NEJMoa1903835 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
