

Time Trends and Variation in the Use of Active Surveillance for Management of Low-risk Prostate Cancer in the US
- PMID: 36862409
- PMCID: PMC9982696
- DOI: 10.1001/jamanetworkopen.2023.1439
Time Trends and Variation in the Use of Active Surveillance for Management of Low-risk Prostate Cancer in the US
Abstract
Importance: Active surveillance (AS) is endorsed by clinical guidelines as the preferred management strategy for low-risk prostate cancer, but its use in contemporary clinical practice remains incompletely defined.
Objective: To characterize trends over time and practice- and practitioner-level variation in the use of AS in a large, national disease registry.
Design, setting, and participants: This retrospective analysis of a prospective cohort study included men with low-risk prostate cancer, defined as prostate-specific antigen (PSA) less than 10 ng/mL, Gleason grade group 1, and clinical stage T1c or T2a, newly diagnosed between January 1, 2014, and June 1, 2021. Patients were identified in the American Urological Association (AUA) Quality (AQUA) Registry, a large quality reporting registry including data from 1945 urology practitioners at 349 practices across 48 US states and territories, comprising more than 8.5 million unique patients. Data are collected automatically from electronic health record systems at participating practices.
Exposures: Exposures of interest included patient age, race, and PSA level, as well as urology practice and individual urology practitioners.
Main outcomes and measures: The outcome of interest was the use of AS as primary treatment. Treatment was determined through analysis of electronic health record structured and unstructured clinical data and determination of surveillance based on follow-up testing with at least 1 PSA level remaining greater than 1.0 ng/mL.
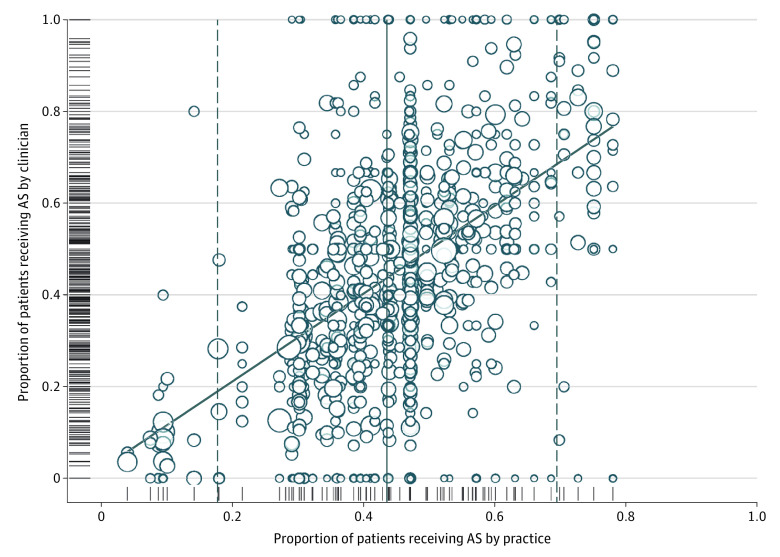
Results: A total of 20 809 patients in AQUA were diagnosed with low-risk prostate cancer and had known primary treatment. The median age was 65 (IQR, 59-70) years; 31 (0.1%) were American Indian or Alaska Native; 148 (0.7%) were Asian or Pacific Islander; 1855 (8.9%) were Black; 8351 (40.1%) were White; 169 (0.8%) were of other race or ethnicity; and 10 255 (49.3%) were missing information on race or ethnicity. Rates of AS increased sharply and consistently from 26.5% in 2014 to 59.6% in 2021. However, use of AS varied from 4.0% to 78.0% at the urology practice level and from 0% to 100% at the practitioner level. On multivariable analysis, year of diagnosis was the variable most strongly associated with AS; age, race, and PSA value at diagnosis were all also associated with odds of surveillance.
Conclusions and relevance: This cohort study of AS rates in the AQUA Registry found that national, community-based rates of AS have increased but remain suboptimal, and wide variation persists across practices and practitioners. Continued progress on this critical quality indicator is essential to minimize overtreatment of low-risk prostate cancer and by extension to improve the benefit-to-harm ratio of national prostate cancer early detection efforts.
Conflict of interest statement
Figures


Comment in
-
Urologic Oncology: Prostate Cancer.J Urol. 2023 Aug;210(2):381-382. doi: 10.1097/JU.0000000000003541. Epub 2023 May 18. J Urol. 2023. PMID: 37199093 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
