

Evolution of long-term vaccine-induced and hybrid immunity in healthcare workers after different COVID-19 vaccine regimens
- PMID: 36863347
- PMCID: PMC9933851
- DOI: 10.1016/j.medj.2023.02.004
Evolution of long-term vaccine-induced and hybrid immunity in healthcare workers after different COVID-19 vaccine regimens
Abstract
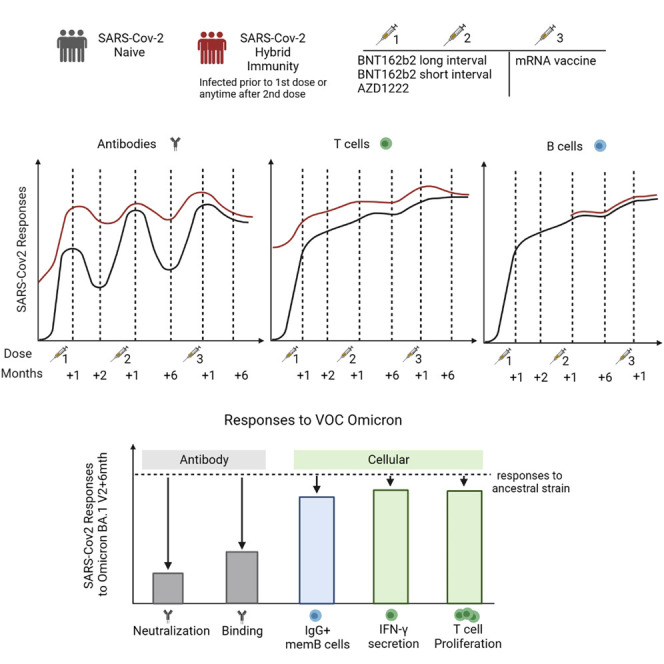
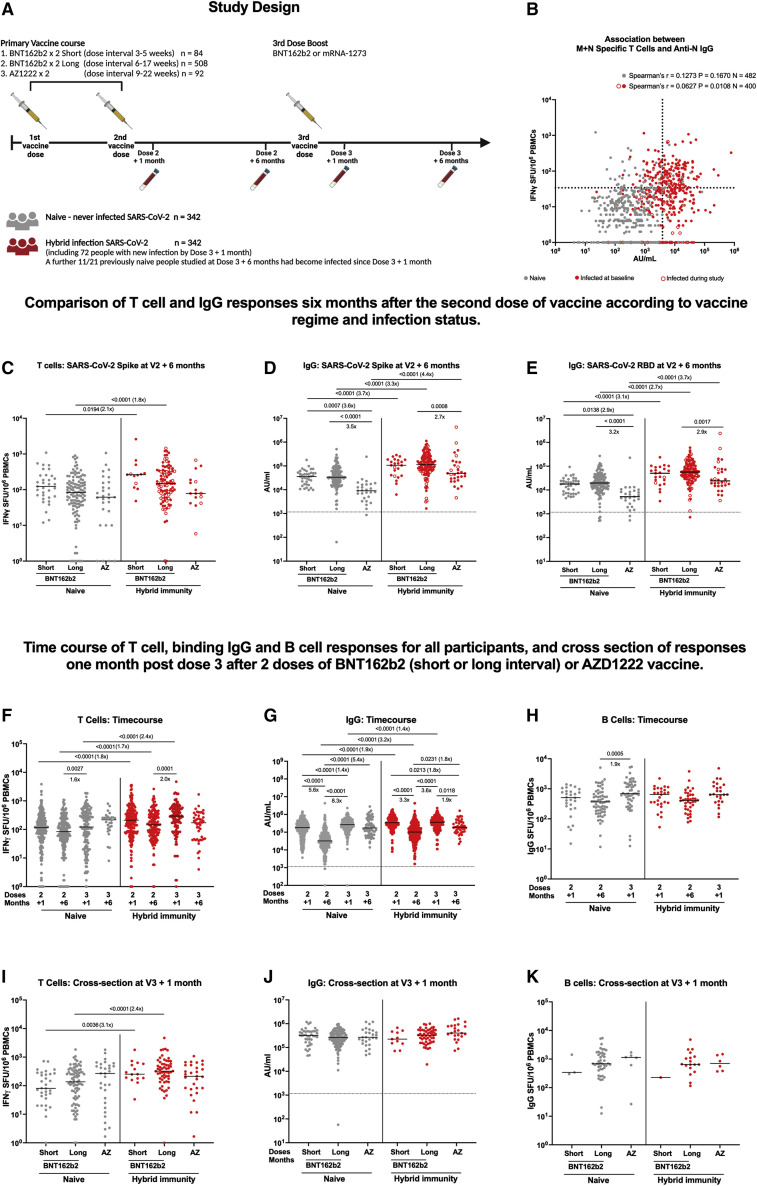
Background: Both infection and vaccination, alone or in combination, generate antibody and T cell responses against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). However, the maintenance of such responses-and hence protection from disease-requires careful characterization. In a large prospective study of UK healthcare workers (HCWs) (Protective Immunity from T Cells in Healthcare Workers [PITCH], within the larger SARS-CoV-2 Immunity and Reinfection Evaluation [SIREN] study), we previously observed that prior infection strongly affected subsequent cellular and humoral immunity induced after long and short dosing intervals of BNT162b2 (Pfizer/BioNTech) vaccination.
Methods: Here, we report longer follow-up of 684 HCWs in this cohort over 6-9 months following two doses of BNT162b2 or AZD1222 (Oxford/AstraZeneca) vaccination and up to 6 months following a subsequent mRNA booster vaccination.
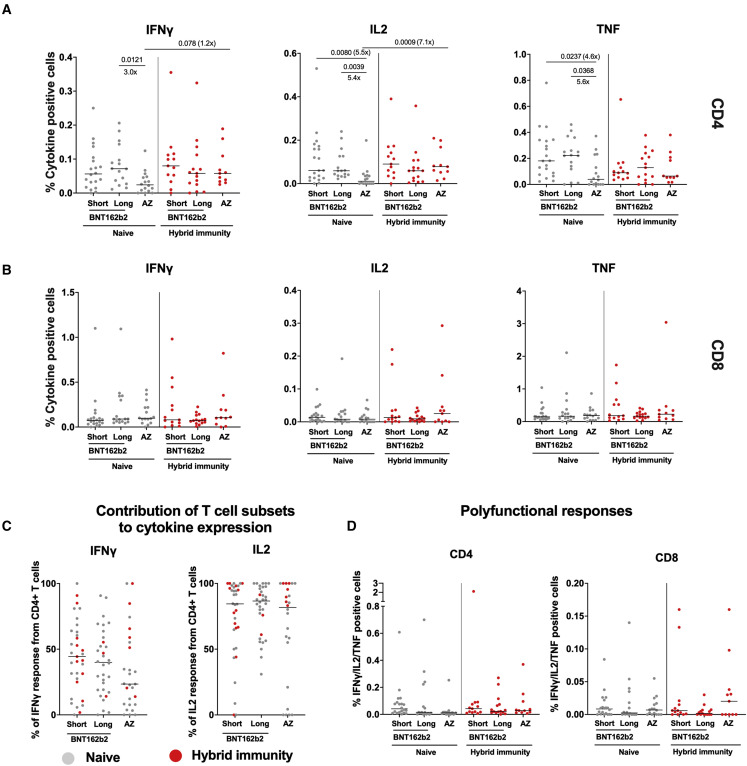
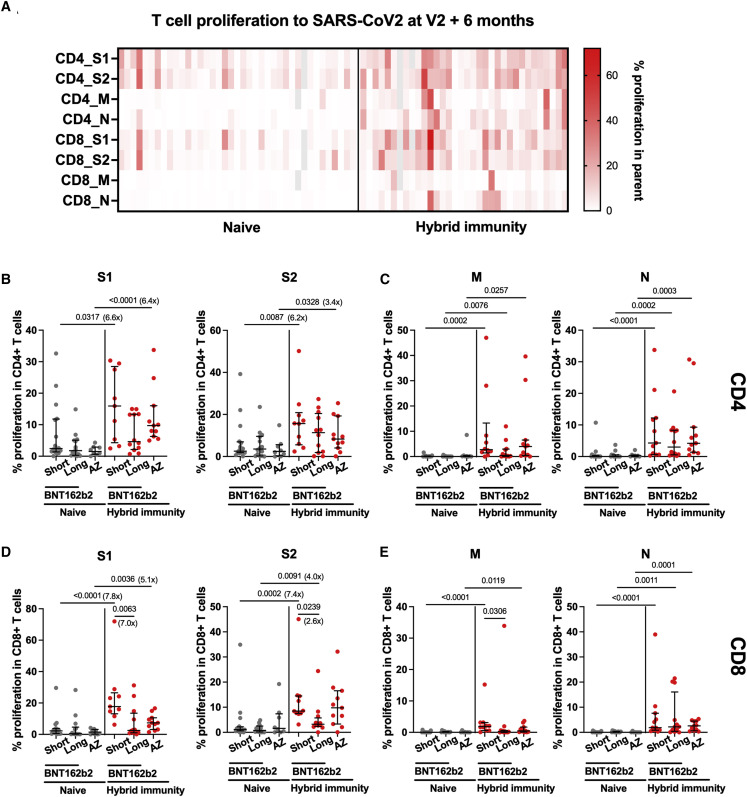
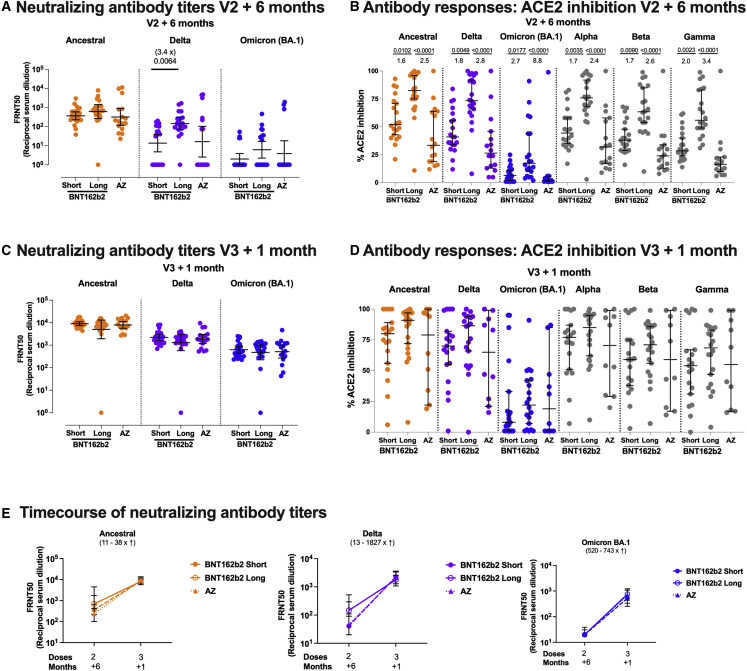
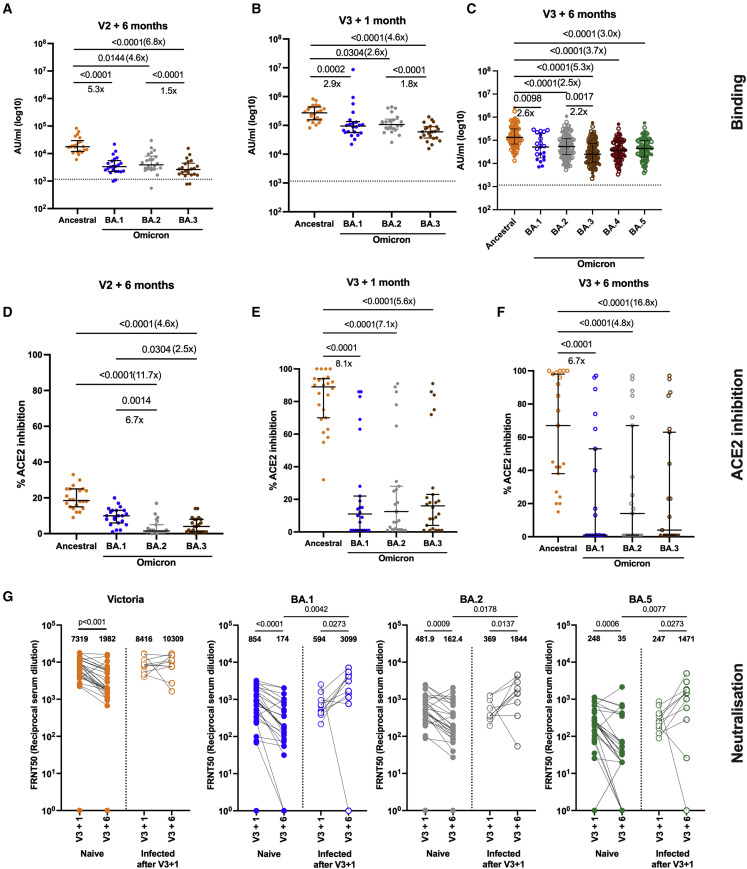
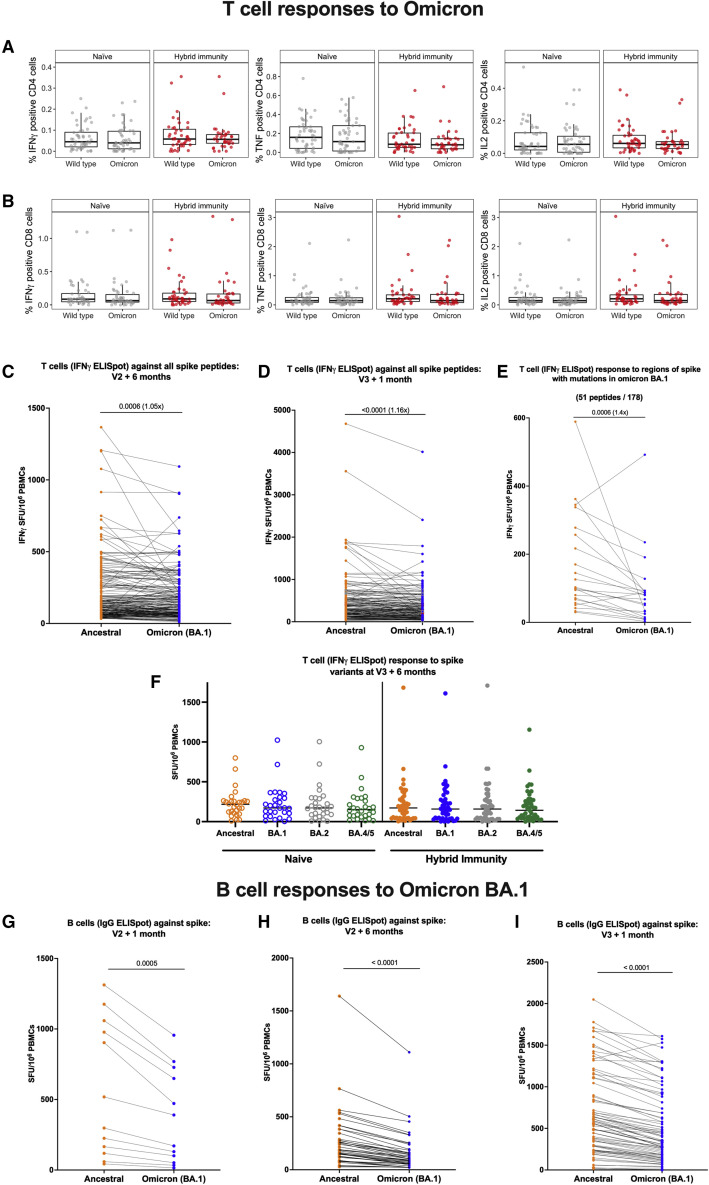
Findings: We make three observations: first, the dynamics of humoral and cellular responses differ; binding and neutralizing antibodies declined, whereas T and memory B cell responses were maintained after the second vaccine dose. Second, vaccine boosting restored immunoglobulin (Ig) G levels; broadened neutralizing activity against variants of concern, including Omicron BA.1, BA.2, and BA.5; and boosted T cell responses above the 6-month level after dose 2. Third, prior infection maintained its impact driving larger and broader T cell responses compared with never-infected people, a feature maintained until 6 months after the third dose.
Conclusions: Broadly cross-reactive T cell responses are well maintained over time-especially in those with combined vaccine and infection-induced immunity ("hybrid" immunity)-and may contribute to continued protection against severe disease.
Funding: Department for Health and Social Care, Medical Research Council.
Keywords: COVID vaccine; COVID-19; SARS-CoV-2; T cells; Translation to population health; antibody; immunity.
Copyright © 2023. Published by Elsevier Inc.
Conflict of interest statement
Declaration of interests S.J.D. is a Scientific Advisor to the Scottish Parliament on COVID-19, for which she receives a fee. A.J.P. is Chair of UK Department of Health and Social Care’s (DHSC) Joint Committee on Vaccination and Immunisation (JCVI) but does not participate in policy decisions on COVID-19 vaccines. He was previously a member of the WHO’s SAGE. The views expressed in this article do not necessarily represent the views of DHSC, JCVI, or WHO. A.J.P. is chief investigator on clinical trials of Oxford University’s COVID-19 vaccine funded by NIHR. Oxford University has entered a joint COVID-19 vaccine development partnership with AstraZeneca. G.S. sits on the GSK Vaccines Scientific Advisory Board and is a founder member of RQ Biotechnology.
Figures
References
-
- UK Health Security Agency . UK Health Security Agency; 2022. COVID-19 Vaccine Surveillance Report: 12 May 2022 (Week 19)
-
- Tartof S.Y., Slezak J.M., Fischer H., Hong V., Ackerson B.K., Ranasinghe O.N., Frankland T.B., Ogun O.A., Zamparo J.M., Gray S., et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet. 2021;398:1407–1416. - PMC - PubMed
-
- Hall V.J., Foulkes S., Charlett A., Atti A., Monk E.J.M., Simmons R., Wellington E., Cole M.J., Saei A., Oguti B., et al. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN) Lancet. 2021;397:1459–1469. - PMC - PubMed
-
- Hall V.J., Foulkes S., Saei A., Andrews N., Oguti B., Charlett A., Wellington E., Stowe J., Gillson N., Atti A., et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): a prospective, multicentre, cohort study. Lancet. 2021;397:1725–1735. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 110058/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/W02067X/1/MRC_/Medical Research Council/United Kingdom
- FS/18/52/33808/BHF_/British Heart Foundation/United Kingdom
- MR/X009297/1/MRC_/Medical Research Council/United Kingdom
- COV19-RECPLAS/DH_/Department of Health/United Kingdom
- PG/11/116/29,288/BHF_/British Heart Foundation/United Kingdom
- 211153/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- MR/X001598/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_0025/12/MRC_/Medical Research Council/United Kingdom
- NIHR300791/DH_/Department of Health/United Kingdom
- PG/11/116/29288/BHF_/British Heart Foundation/United Kingdom
- 204721/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 110,110Z/15/Z/WT_/Wellcome Trust/United Kingdom
- MR/W020564/1/MRC_/Medical Research Council/United Kingdom
- NIHR200907/DH_/Department of Health/United Kingdom
- 205228/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 090532/Z/09/Z/WT_/Wellcome Trust/United Kingdom
- WT109965MA/WT_/Wellcome Trust/United Kingdom
- D43 TW009127/TW/FIC NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
