

A deep-learning algorithm to classify skin lesions from mpox virus infection
- PMID: 36864252
- PMCID: PMC10033450
- DOI: 10.1038/s41591-023-02225-7
A deep-learning algorithm to classify skin lesions from mpox virus infection
Abstract
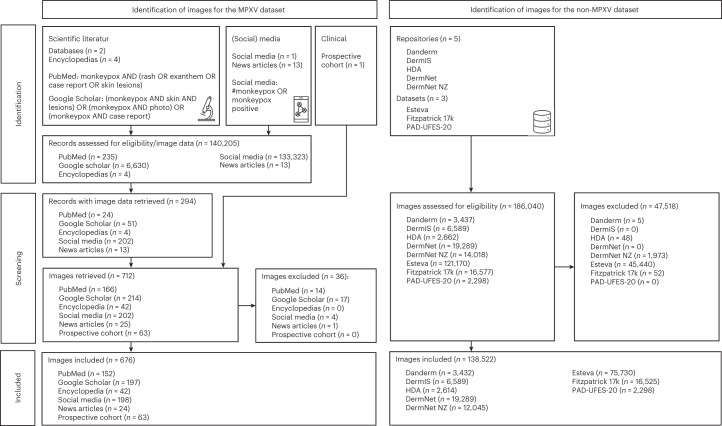
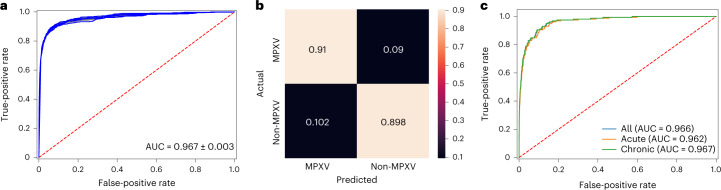
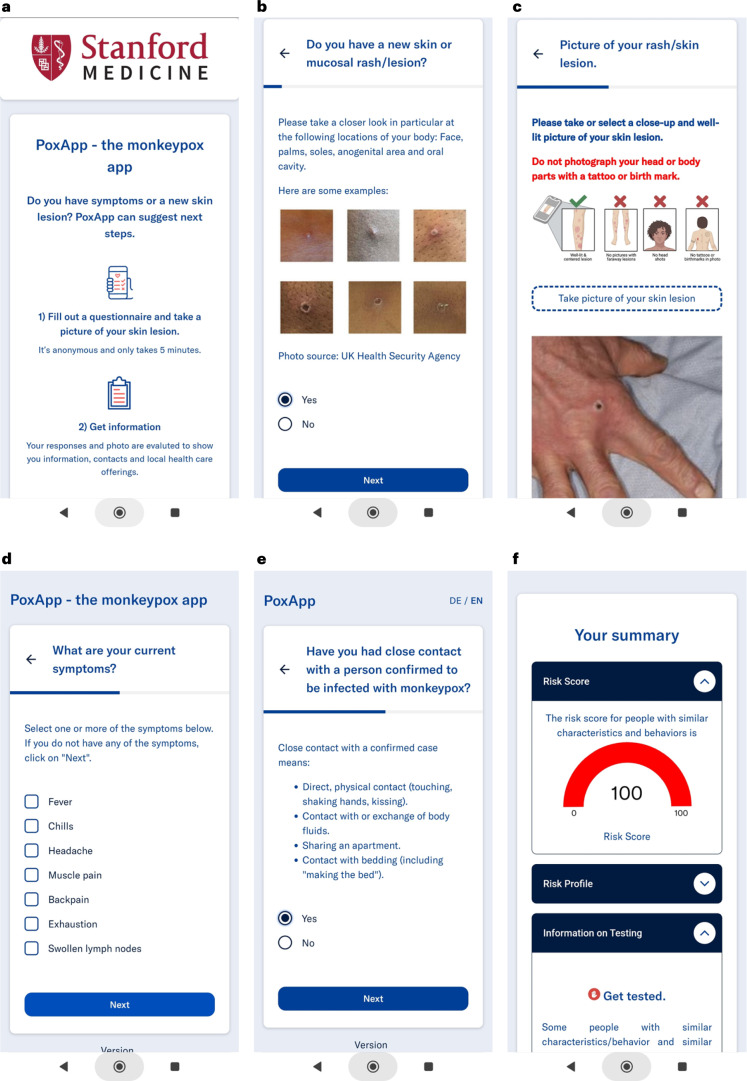
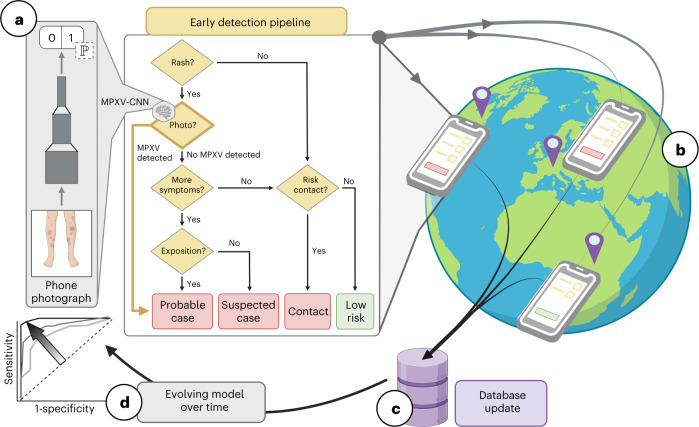
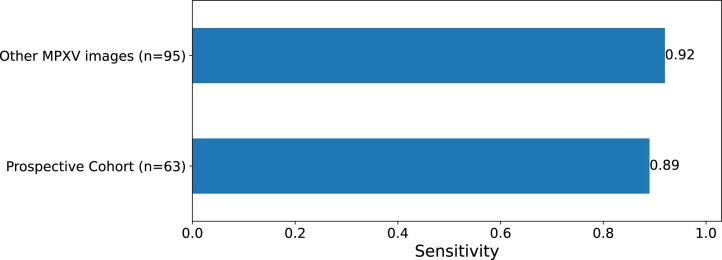
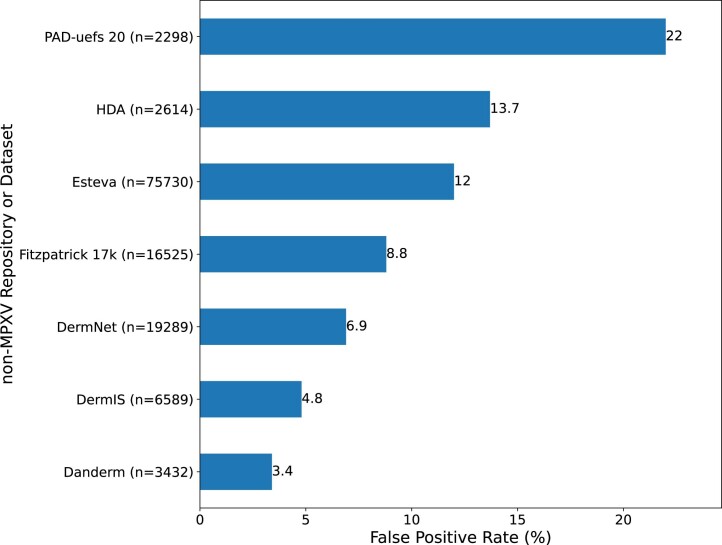
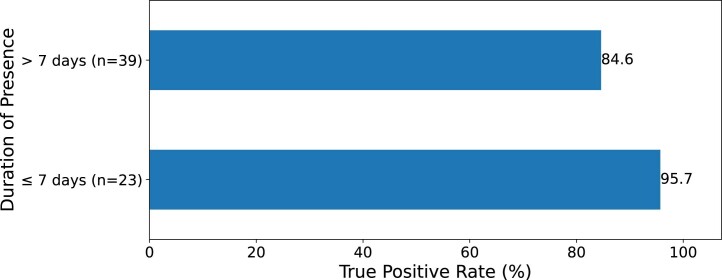
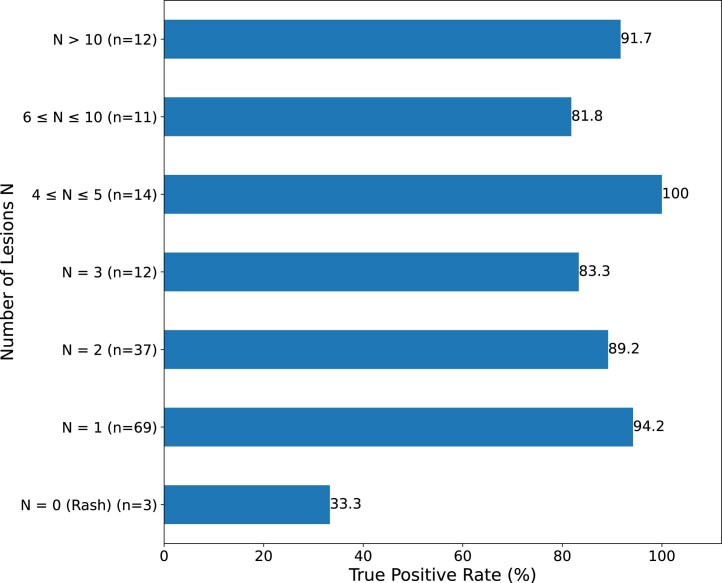
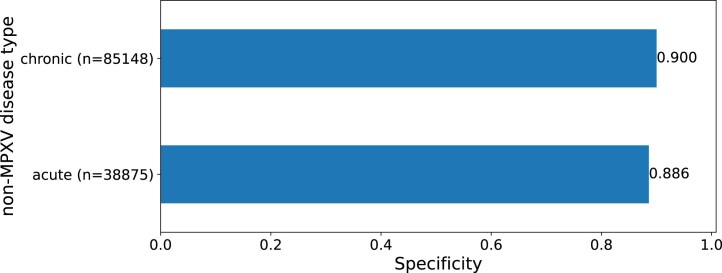
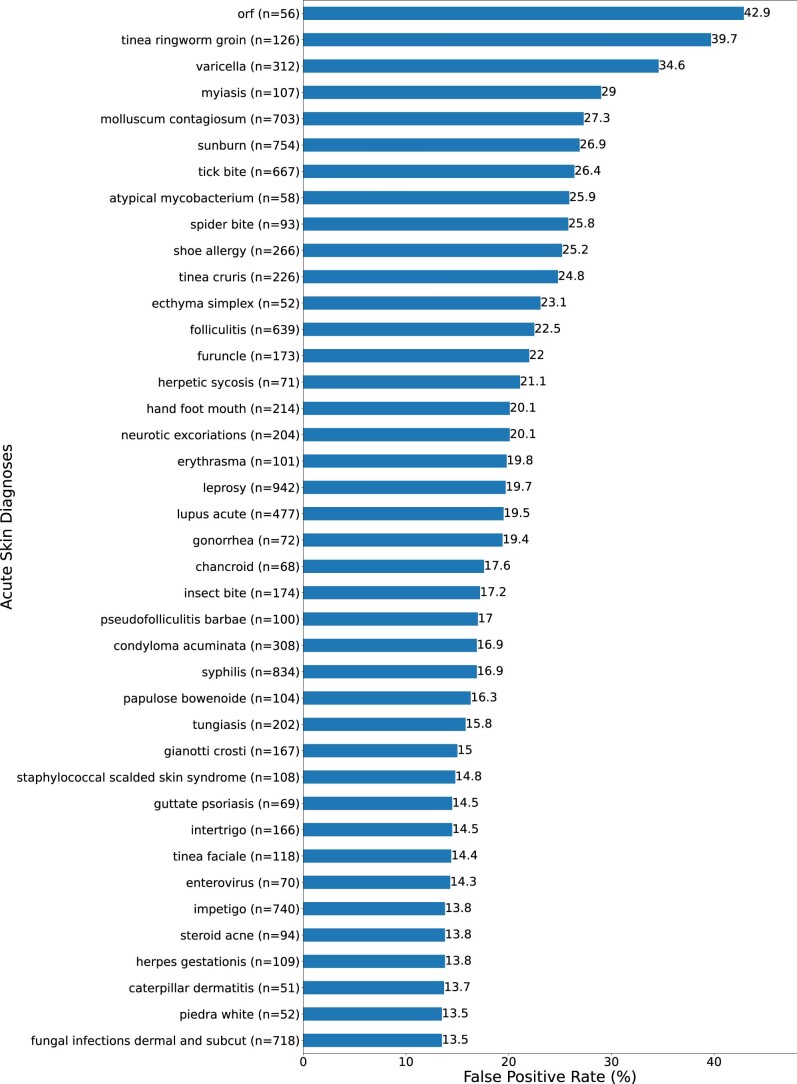
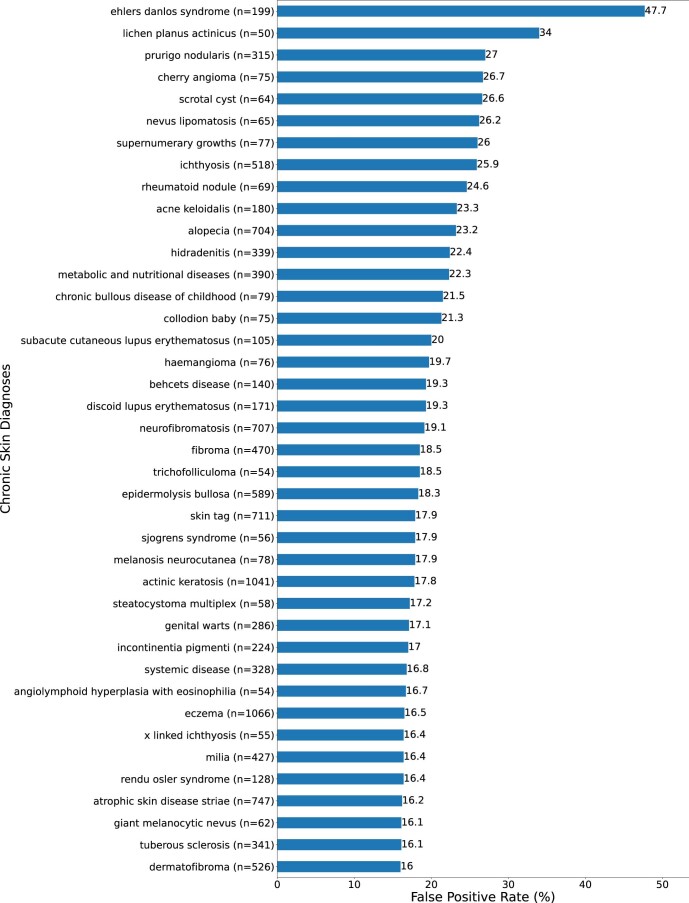
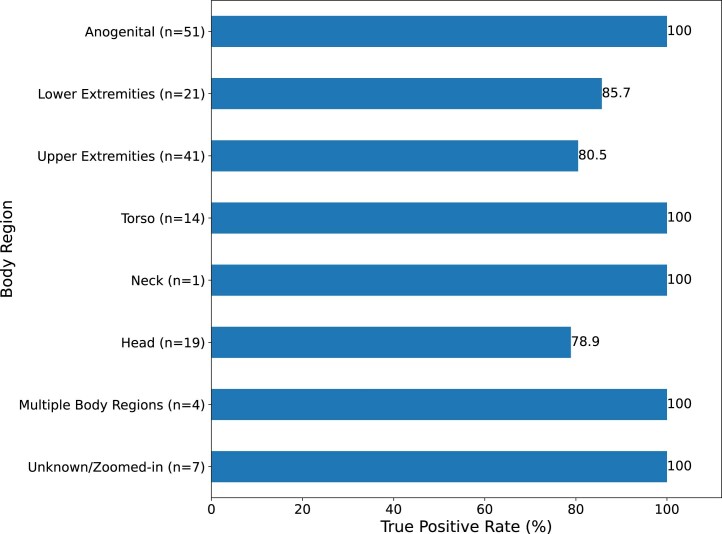
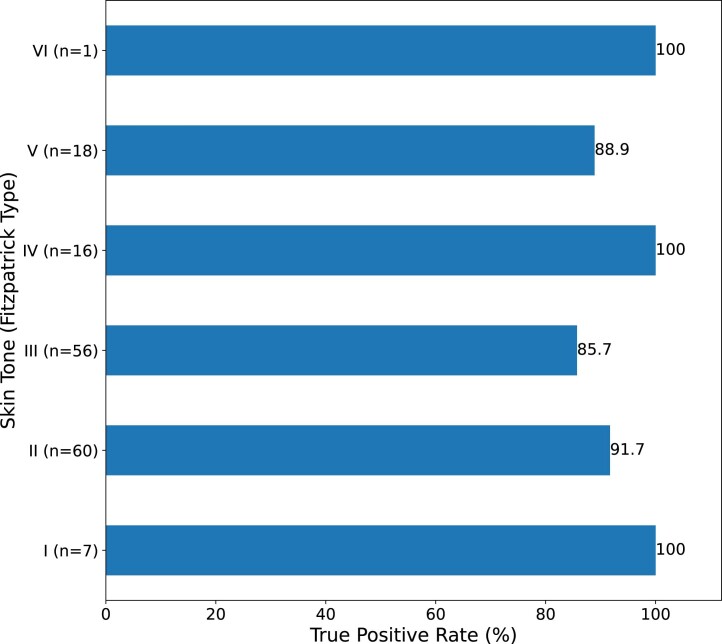
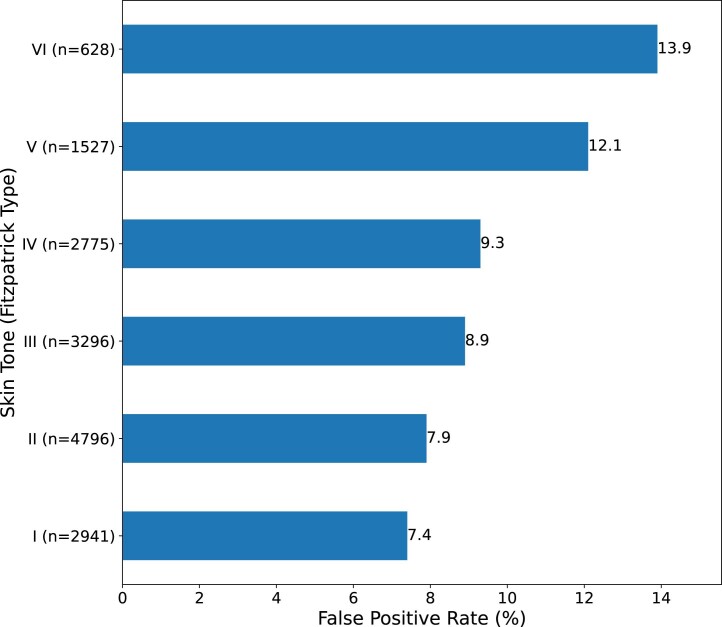
Undetected infection and delayed isolation of infected individuals are key factors driving the monkeypox virus (now termed mpox virus or MPXV) outbreak. To enable earlier detection of MPXV infection, we developed an image-based deep convolutional neural network (named MPXV-CNN) for the identification of the characteristic skin lesions caused by MPXV. We assembled a dataset of 139,198 skin lesion images, split into training/validation and testing cohorts, comprising non-MPXV images (n = 138,522) from eight dermatological repositories and MPXV images (n = 676) from the scientific literature, news articles, social media and a prospective cohort of the Stanford University Medical Center (n = 63 images from 12 patients, all male). In the validation and testing cohorts, the sensitivity of the MPXV-CNN was 0.83 and 0.91, the specificity was 0.965 and 0.898 and the area under the curve was 0.967 and 0.966, respectively. In the prospective cohort, the sensitivity was 0.89. The classification performance of the MPXV-CNN was robust across various skin tones and body regions. To facilitate the usage of the algorithm, we developed a web-based app by which the MPXV-CNN can be accessed for patient guidance. The capability of the MPXV-CNN for identifying MPXV lesions has the potential to aid in MPXV outbreak mitigation.
© 2023. The Author(s).
Conflict of interest statement
I.B. consults to BlueDot, a social benefit corporation that tracks emerging infectious diseases, and to the NHL Players’ Association. The authors declare no competing interests.
Figures
Comment in
-
Deep learning for Mpox: Advances, challenges, and opportunities.Med. 2023 May 12;4(5):283-284. doi: 10.1016/j.medj.2023.04.002. Med. 2023. PMID: 37178679 Free PMC article.
References
-
- World Health Organization. Second meeting of the International Health Regulations (2005) (IHR) Emergency Committee regarding the multi-country outbreak of monkeypox. https://www.who.int/news/item/23-07-2022-second-meeting-of-the-internati... (2022).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
