

Codon-specific KRAS mutations predict survival benefit of trifluridine/tipiracil in metastatic colorectal cancer
- PMID: 36864254
- PMCID: PMC10033412
- DOI: 10.1038/s41591-023-02240-8
Codon-specific KRAS mutations predict survival benefit of trifluridine/tipiracil in metastatic colorectal cancer
Abstract
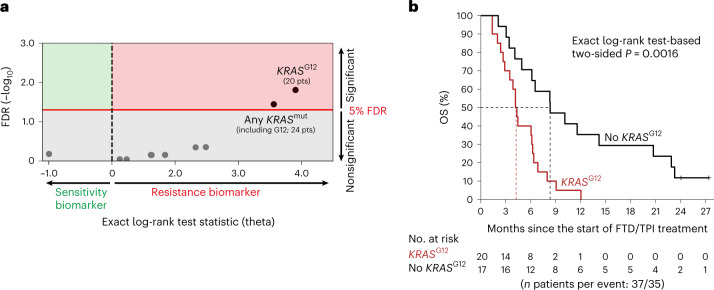
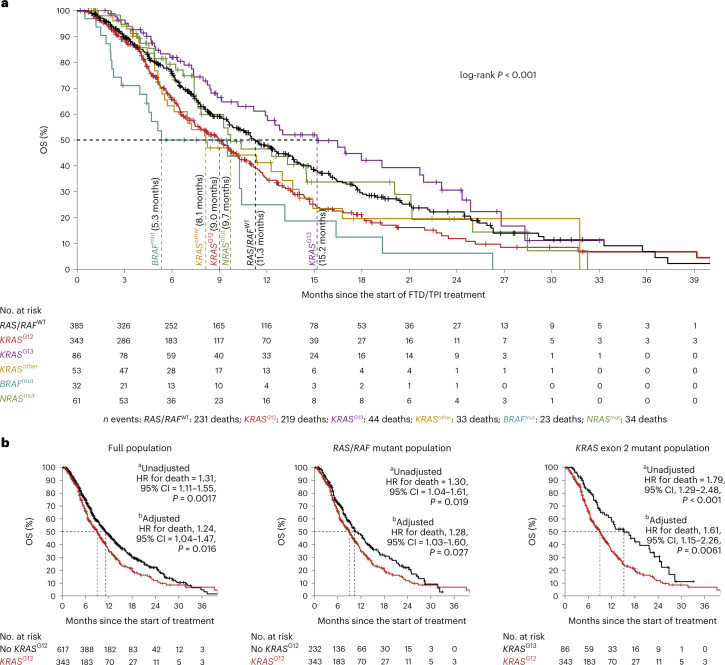
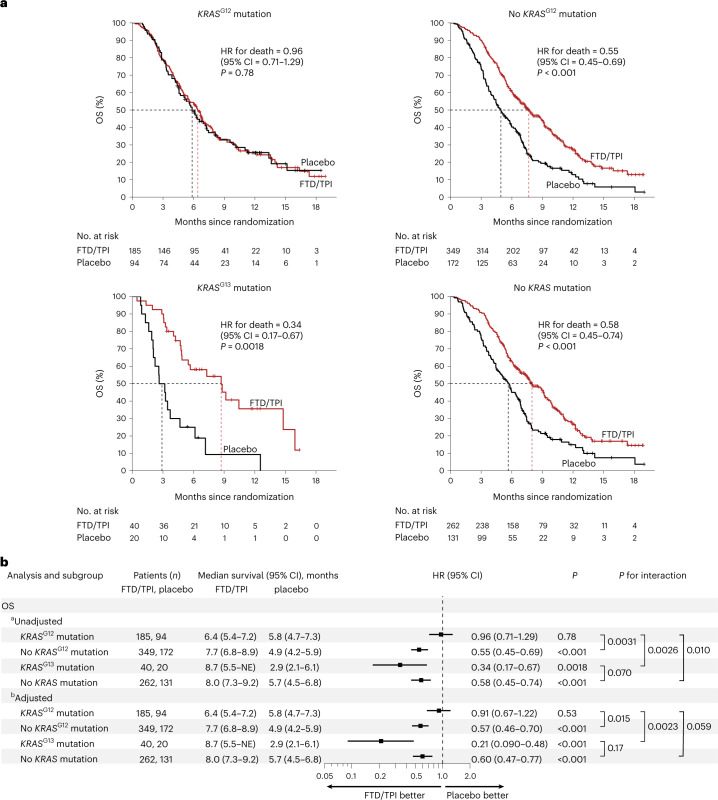
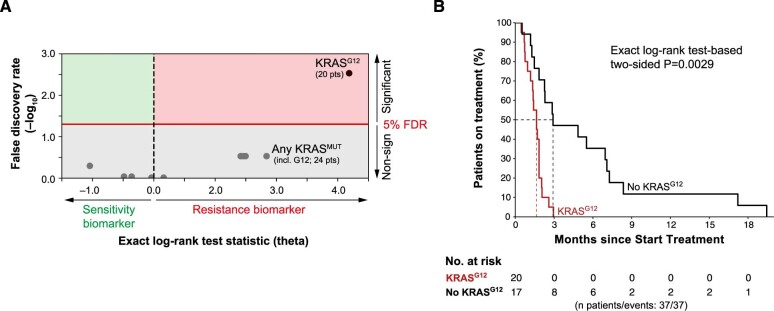
Genomics has greatly improved how patients with cancer are being treated; however, clinical-grade genomic biomarkers for chemotherapies are currently lacking. Using whole-genome analysis of 37 patients with metastatic colorectal cancer (mCRC) treated with the chemotherapy trifluridine/tipiracil (FTD/TPI), we identified KRAS codon G12 (KRASG12) mutations as a potential biomarker of resistance. Next, we collected real-world data of 960 patients with mCRC receiving FTD/TPI and validated that KRASG12 mutations were significantly associated with poor survival, also in analyses restricted to the RAS/RAF mutant subgroup. We next analyzed the data of the global, double-blind, placebo-controlled, phase 3 RECOURSE trial (n = 800 patients) and found that KRASG12 mutations (n = 279) were predictive biomarkers for reduced overall survival (OS) benefit of FTD/TPI versus placebo (unadjusted interaction P = 0.0031, adjusted interaction P = 0.015). For patients with KRASG12 mutations in the RECOURSE trial, OS was not prolonged with FTD/TPI versus placebo (n = 279; hazard ratio (HR) = 0.97; 95% confidence interval (CI) = 0.73-1.20; P = 0.85). In contrast, patients with KRASG13 mutant tumors showed significantly improved OS with FTD/TPI versus placebo (n = 60; HR = 0.29; 95% CI = 0.15-0.55; P < 0.001). In isogenic cell lines and patient-derived organoids, KRASG12 mutations were associated with increased resistance to FTD-based genotoxicity. In conclusion, these data show that KRASG12 mutations are biomarkers for reduced OS benefit of FTD/TPI treatment, with potential implications for approximately 28% of patients with mCRC under consideration for treatment with FTD/TPI. Furthermore, our data suggest that genomics-based precision medicine may be possible for a subset of chemotherapies.
© 2023. The Author(s).
Conflict of interest statement
E.E.V. reports research grants from Roche, Pfizer, GSK, Novartis, Merck, Bristol Myers Squibb, AstraZeneca, Amgen, Bayer, Sanofi, Seagen, Janssen, Eisai, Ipsen and Lilly. He is a founder, strategic advisor and shareholder of MOSAIC Therapeutics and nonexecutive, independent director and shareholder of Sanofi, all outside the submitted work. L.F.A.W. reports grants from Genmab, outside the submitted work. A.C. received grant consultancy fees from MSD, AstraZeneca, Oncoc4 and IQVIA. He also declares speaker’s fees from Eisai and AstraZeneca. A.P. received personal fees from Lilly, Servier, Merck, Amgen, Bristol Myers Squibb and MSD. A.T. declares speaker bureau fees from Bristol Myers Squibb and Servier. C.S. received honoraria from the speaker bureau at Servier. D.J.P. received lecture fees from ViiV Healthcare, Bayer Healthcare, Bristol Myers Squibb, Roche, Eisai and the Falk Foundation, travel expenses from Bristol Myers Squibb and Bayer Healthcare, consulting fees for Mina Therapeutics, H3B, Eisai, Roche, DaVolterra, Mursla, Exact Sciences, Avamune and AstraZeneca and research funding (to institution) from MSD, Bristol Myers Squibb and GSK. F.G. received honoraria for speaker/advisory roles from Servier, Lilly, IQVIA, Merck Serono, Bayer, Amgen and Bristol Myers Squibb outside the present work. F.M. received fees from the speaker bureaux of Servier, Amgen, Novartis, MSD and Merck. G.T. took part in the advisory boards for Bristol Myers Squibb, AstraZeneca, MSD, Merck and Servier. J.G. received honoraria for educational events organized by Servier. L.S. received speaker and consultancy fees from MSD, AstraZeneca, Servier, Bayer, Merck, Amgen and Pierre-Fabre. M.G.R. received consultancy fees from Roche. M.G. received grants and advisory board fees from Merck, Servier, Lilly, Amgen and Italfarmaco. N.L.V. received fees and honoraria from Eisai, MSD, Roche, Novartis, AstraZeneca, GSK, Pfizer, Gentili and Lilly. N.V. received honoraria from Merck Serono, Pfizer, Bayer, Lilly and Servier, consultancy fees from BenevolentAI and grants (institutional) from Roche and BenevolentAI. N.Z. declares personal fees from Bayer and Eisai. O.G. reports consulting fees from Eisai, Lilly, MSD and Seagen and payment or honoraria for lectures, presentations, speaker bureaux fees, manuscript writing or educational events from Novartis, Lilly and Eisai. P.R. received grants from Bayer and Sanofi, honoraria for advisory boards from AstraZeneca, Eisai, Servier and Sirtex, speaking fees from Amgen, Boston Scientific, HMP Education, Eisai, Roche and Servier and travel conference support from Bayer, Roche, Ipsen and Servier. R.G. took part in advisory boards for Merck, Amgen, Servier and Bayer. R.B. declares consultancies, advisory board roles and/or institutional donations from AstraZeneca, Boehringer Ingelheim, Novartis, MSD, Otsuka, Lully, Roche, Amgen, GSK and Eisai. T.I. received honoraria for educational symposia run by Servier. All other authors declare no competing interests.
Figures








Comment in
-
Mutations linked to chemotherapy resistance in colorectal cancer.Nat Rev Gastroenterol Hepatol. 2023 May;20(5):269. doi: 10.1038/s41575-023-00772-5. Nat Rev Gastroenterol Hepatol. 2023. PMID: 37012321 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
